
Hong Kong Journal of Psychiatry (1998) 8 (1) 3-8
Mental Health and Services
Summary
A study of Chinese health statistics demonstrates a number of very unusual features in the mental health profiles of women e.g. that there are more completed suicides amongst women than men, and more women than men are diagnosed with schizophrenia, although psychiatric hospital beds are disproportionately occupied by men. This article examines how the social, economic and political environment impinge, at the macro-level, on access to health care and at the micro-level on the experience and interpretation of distress.
Key words: China, women, mental health, suicide, schizophrenia
INTRODUCTION
The health and mental health profiles of men and woman in China show significant differences in some respects. On the face of it, women seem to do rather better. In line with the rest of the world where women have equal access to health and survival resources women in China outlive men by over four years (Work! Bank, 1989). Chinese men have a fifteen percent chance of dying between the ages of 15 and 60 whereas for women it is about an 11percent chance.
Yet viewed from a comparative perspective these figures do not present such a positive picture. Their probabilities of death place Chinese men in the middle of fifty-five countries but only eleven countries have a higher probability of death for women (World Bank, 1992). A recent World Bank/WHO collaborative study found that the years of life lived with a disability were 15 per cent lower for men in China than for women (Murray, et al., 1994). For the first time in 1993 'mental illness' was listed (at tenth place) in The China Health Year Book among the most common causes of deaths. It was there because of the suicide rate amongst women which ranks as the ninth most common cause of death among women. In cities 'mental illness' is responsible for 6.82/100,000 female deaths. 'Mental illness' does not feature in the list of the 10 leading causes of death for men.
THE FOURTH MOUNTAIN
Such differences in the health and ill-health of men and women cannot be solely explained by differences in biology. Social, political and economic factors also impinge. Mao Zedong once said that all Chinese carried three mountains on their backs, imperialism, feudalism and capitalism; but women carried a fourth mountain, male supremacy. The belief in the acceptance of male supremacy is deeply entrenched in Chinese culture (as it is in a number of others). After Liberation, the Communist Party made strenuous efforts to eliminate the conditions in which male supremacy thrived. The new Constitution that they introduced closely followed by the new Marriage Law revolutionized the legal basis of the relationship between men and women.
Like others before them, however, the Chinese government is currently faced with the realization that it is a relatively easy matter to change the law but an extraordinarily complex and lengthy business to change what people believe and how they behave. For as long as the government maintained strict centralized control of the country, they were in a position to enforce their policies of gender equality. For instance when jobs were centrally allocated enterprises had to accept women in management positions. With the advent of the new economic opportunities from the mid-1980s the central government lost effective control of the provinces. By insisting that they become economically independent and responsible for themselves, the government surrendered the most effective weapon in its armoury for enforcing its will. One of the casualties of the government's retreat from centralized control was its gender equality policy which it was no longer in any position to enforce, although the rhetoric remained the same. Thus Ro92n (1987) has argued that the current economic policies being pursued in China to establish a socialist market economy (capitalism in all but name) have done more to disadvantage women than at any time since 1949. Women's liberation and economic development are seen to be in conflict, rather than the first preceding or at least accompanying the latter (Pearson, 1995).
This line of argument may be interesting but how does it affect mental health? Bernandez (1984) suggests that there are four ways in which social factors can influence women's mental health. Firstly, women are socialized into accepting culturally defined female roles as normal, when in fact they are not, and where non-conformity to these roles is then interpreted as sickness or deviance (Broverman et al., 1987). Secondly, if women clearly are less valued than men this is inevitably going to have an affect on at least some individual psyches. Thirdly, the effects of discrimination in terms of education, employment and so on may lead to bitterness and frustration. Finally, health professionals from whom help is sought may no more be free of the cultural stereotypes of male and female behaviour than laymen (Broverman et al., 1987). Consequently, their intervention may exacerbate the problems of individual women.
It is not difficult to demonstrate that boy preference is still a major influence in Chinese society, with clear effects in health terms. The 'one-child policy' and its consequences have been discussed at length elsewhere (Pearson, 1995; Pearson, 1996; Banister, 1987). Suffice it to say that in the urban areas it has been more easily accepted where the economic cost of raising a child is such that 'one child but a healthy child' makes sense, even if that child is a girl. However, in the rural areas (and 0 around 60 per cent of China is officially classified as .9Jch) the desire for a son continues to be so great as to generate vigorous resistance to population control mea.9..1res. This is clearly demonstrated by population figures. The normal sex ratio at birth is 100 girls to approximately 105-106 boys. Throughout the 1960s and most of the 1970s (when people could have as many children as they liked) this was the case in China. From 1980 it began to change: 1981, 108.5; 1986, 110.9; in 1991, 113.8 (Zheng, Tu, Gu et al., 1993). These are national figures combining urban and rural areas. Greenhalgh et al. (1994) say that for third and higher parity births for the three villages in Shaanxi that they studied, the ratio was 1:1,100. There is general agreement that the reasons for these gross demographic imbalances are due to infanticide, sex-selective abortion and not registering female births. However the various authorities disagree as to the distribution of responsibility between these three causes (Banister, 1987; Aird, 1990; Zeng et al., 1993; Greenhalgh et al., 1994).
Even if girl children survive birth, neglect may also affect their life chances. Ren (1993) points out that in his studies in Shaanxi, girl toddlers chances of surviving childhood are significantly less than boys. He attributes this to the unequal distribution of food, health care and parental supervision. This may also be seen on a national scale, where the mortality rate for boys of five years and under is 6.37 in the cities and 6.88 at the county level. For girls it is 7.58 and 8.38 respectively (Beijing Review, 24-10-94). One might think that, following modern economic theory, scarcity would bring higher value and status. Sadly, in the case of young women, this does not seem to be so. The rise in the kidnap and trafficking of women that has been so prominent a feature in the last 8 years in China is directly attributable to the lack of women of marriageable age in rural areas (Pearson, 1996).
EPIDEMIOLOGICAL DATA ON MENTAL HEALTH
While it is undeniable that the status of women in China, particularly in the urban areas has risen since 1949, the previous discussion makes it clear that understanding of women's mental health status must be placed within a context that takes account of non-biological factors. The most comprehensive study of psychiatric disorder in China is known as the Twelve Centres Epidemiological Survey and was carried out with the advice and assistance of the World Health Orgariization (Co-ordinating Group, 1986; Zhao, 1986). This survey has recently become available in English translation (Cooper and Sartorius, 1996). A revue (in English) of all the surveys in this area carried out in China, up to and including 1990, is contained in Cheung (1991) but it ignores gender differences.
WOMEN AND SCHIZOPHRENIA
The Twelve Centres Epidemiological Survey found that the point prevalence rate for schizophrenia was 6.00/1000 in the urban areas and 3.42/1000 in the rural areas (Shen, 1986). Leff (1988) gives prevalence figures from a variety of countries, ranging from 0.9 - 8.0/1000, suggesting that the Chinese figures are within an expected range. There was a marked gender difference in the Chinese sample. The lifetime prevalence rate for women was 7.07/1000 and for men, 4.33/1000. This difference held good in both urban and rural areas and was significant at the < 0.01 level (Chen, 1986). Thus the rate for women was almost double that for men. Chen attributes these differences to the higher psychological and social burdens that women have to bear.
To the Western eye, one of the most remarkable aspects of the results from the Twelve Centre Epidemiological Survey is that apparently significantly more women than men .9..1ffer from schizophrenia. Phillips and Pearson (1994) have expressed some reservations about case finding in the Twelve Centres Epidemiological Survey in relation to the large urban/rural difference in the occurrence of schizophrenia. The gender differences may also be an artefact of case finding methods. If they reflect a true difference, this would be a most unusual circumstance.
No national statistics are kept of the distribution of psychiatric beds by gender. Even the officially reported numbers of hospital beds are likely to be unreliable (Pearson, 1995). Thus any suggestions must be tentative. However, 1 have visited at least 15 psychiatric hospitals in China and in all those where the provision of beds was a response to the demand from the community, male beds outnumbered female beds by at least 6:4 and sometimes more. This was also found in a study of three psychiatric hospitals in China (Phillips et al. 1990). Thus we have a situation where according to the most scientifically conducted epidemiological study so far there is a significant excess of female patients suffering from schizophrenia, but an equally significant preponderance of beds for males. Between 75-80 per cent of psychiatric hospital beds in China are occupied by people diagnosed as suffering from schizophrenia (both men and women), so these figures are not a reflection of admissions for different illnesses between sexes.
How may this be explained? It is well known that there are certain differences between men and women in the way that they are affected by schizophrenia. Schizophrenia tends to develop up to six years earlier in men than in women and more women than men .9..1ffer their first onset after the age of 40 (Loranger, 1984; Angermeyer and Kuhn, 1988). Several studies have reported a worse prognosis, at least where hospital discharge rates are concerned, in men than in women (Kerdell, 1988). Women have fewer relapses and are less likely to develop a chronic course (Seeman, 1982; Goldstein, 1988). The International Pilot Study (Sartorius et al., 1986) found female sex to be the best predictor of a remittent (versus chronic), course of illness and one of the five best predictors with respect to the percentage of follow-up time which the patients spent in a psychotic state. Overall, men do not respond as well to psychotropic medication, requiring higher doses of medication, which they do not tolerate as well as women; their long term adjustment as measured by such indices as social life, marriage, work record, and general level of functioning is not as good as that of women (Torrey, 1988).
To explain these differences, it has been suggested that estrogen may provide protection through a mechanism not yet understood, or that there may be two different kinds of illness involved, one of which tends to start later and have a more benign course and is prevalent in women; the other to predominate in men, with earlier onset and more damaging long term effects.(Seeman, 1982; Torrey, 1988). As yet the work remains to be done in China that would permit us to know whether the position is the same there in these respects.
One of the likely explanations to account for the excess of men in psychiatric hospitals is the difference in social expectations. The role behaviour associated with being a housewife and mother is possibly easier to maintain in the private domain of the family than that associated with being a breadwinner, a success in the marketplace. Women's domestic survival skills outside the hospital are likely to be higher than those of men. In research I carried out in a hospital for long-term psychiatric patients in southern China 40.8 per cent of women were 'ever-married' but only 10.2 per cent of men (significant at the < 0.0001 level). In a hospital for acutely ill psychiatric patients in Beijing, in a comparison of an admission ward for men and another for women, I found that 48 per cent of the men were 'never-married' but only 27 per cent of the women (significant at the < 0.05 level). Part of this difference may be explained by the fact that schizophrenia develops later in women and they marry earlier, certainly in China. Thus their symptoms- may not become apparent until after they are married. Under these circumstances, once parents die men may have no effective family with whom they can live and lack the necessary skills to care for themselves.
Another effect that gender role expectation can have on bed occupation patterns was suggested by several Chinese psychiatrists, who thought that women feel a greater sense of responsibility towards parents, husbands and children and are consequently more reluctant to be admitted and tend to stay for shorter periods of time (at least in the acute sector). The obverse of this is that families cannot function very efficiently without the mother/wife in the house, so that pressure is put on women to return home as quickly as possible. Men on the other hand particularly those working in state enterprises and covered by health insurance, are pleased to be relieved of work and tend to prolong their stays.
In both hospital studies, it became apparent that there were significant differences regarding the payment status of men and women. In the long-term hospital 19.4 per cent of all the men were supported by health insurance provided by their employer. This was true of only 10 per cent of all the women. Thus proportionately more women were 'charity' cases or having to be supported by their families.
Evidence from the acute hospital fleshes out this picture. At this hospital many treatments were offered in addition to the basic 'bed, board and medication' arrangement, and were charged for separately. These treatments included lasar therapy, music therapy, acupuncture, psychotherapy, occupational therapy, behaviour therapy and ECT. Only in the last two was there no significant difference between men and women, suggesting that they were being given on the basis of need rather than ability to pay. The overall difference in the cost of treatment between men (Rmb. 1,500) and women (Rmb. 750) was significant at the < 0.0001 level. This suggests that men had more health insurance and/or that families were more willing to pay inflated costs for men than for women. Interestingly, in the long term hospital where the monthly costs were all inclusive, very little difference was detected between the treatment offered to men and women. Phillips et al. (1990) found that length of stay was most significantly related to whether hospital costs were being met by the family or by health insurance. Neither diagnosis nor severity of the condition were as important. In a situation where women are: less often covered by health insurance, given less priority in access to family finances, needed for the smooth running of the household, and are thought to be more easily contained when they are in an excitable or aggressive state, it is not surprising to find that there are fewer psychiatric hospital beds for women in comparison with men.
WOMEN AND DEPRESSION
The lifetime prevalence rate of schizophrenia is seven times higher than that for affective disorder (including bi-polar disorder) in China. The point prevalence rate is 13 times higher. Only 29 cases of affective disorder (female and male) were found in the overall sample of 38,136 in the Twelve Centres Epidemiological Survey. By Western standards this was astonishingly low. However, there were marked gender differences. The point prevalence male/female ratio was 1:1.35 for affective psychosis. The male/female ratio for reactive psychosis was 1:3.4 (Zhao, 1986). Figures given in Chen et al. (1993) allow us to make comparisons with a Chinese population in Hong Kong. Using DSM3, the authors also found that major depressive disorder and dysthymic disorder were female dominated at the <0.05 level of significance. However, they found no gender differences in the categories of schizophrenia and bi-polar disorder.
It could be argued that the greater prevalence of depression in women in both Western countries (Miles 1987· Belle· 1982· Brown and Harris, 1978) and Chinese societies is an indication that the tendency to develop depression is biologically based. An equally plausible hypothesis is that women, sharing a disadvantaged status, have more to be depressed about. In support of this view, McGuffin and Katz (1989) were unequivocal in stating that the findings from their study led them to the conclusion that most of the gender differences between the sexes regarding the prevalence of depression are due to environmental factors.
The tendency of Chinese doctors to over-diagnose schizophrenia and under diagnose depression and bi-polar disorder is well documented (Liu, 1980; U 83; Yan and Xiang, 1984; Yuan, 1987; Zhao, 1986; Cheung 1991). This is also my impression based on reading hundreds of case files and interviewing with Chinese psychiatrists. It has been suggested that someone who is quietly depressed, withdrawn and uncommunicative is relatively acceptable in a Chinese society that values self-contained and decorous behaviour (Tseng, 1973; Lin, 1981). Those that come to thenotice of doctors are those whose behaviour brings them to public attention.
SUICIDE
This argument is certainly plausible bodies not mean that depression does not exist, only that it goes undetected. Evidence to support this view comes from an examination of suicide statistics which have only relatively recently become available for China, as the topic is one considered highly sensitive by the Chinese government (Pritchard, 1996). The top three causes of injury death in China are suicide (33 percent), motor vehicle crashes (16 per cent) and drowning (14 per cent). In America, death by suicide accounts for 20 per cent of all injury deaths (Li and Baker, 1991).
There is also a sharp difference between the urban and rural suicide rates; 10.00 v 27.7/100,000. There is a marked peak of female suicides in the age bracket 20·24 and among this cohort the suicide rate among women is five times greater in the rural areas than in the urban areas (78.3 v L5.9/100,000) The same pattern is seen among Chinese males in the same age bracket. The rural suicide rate is four times that of the urban areas, 40.7 v 9.9/100,000. Furthermore, Li and Baker (1991) point out that the rural population were under-represented in the sample (43 per cent), when it is usually accepted that at least 60 per cent of the Chinese population are classified as rural. This means that the rural suicide rate is probably higher than reported.
Such high levels of suicide must reflect the social, cultural and economic changes that Chinese society is facing. Such issues seem to bite hardest in the rural areas generally and young women in particular, among whom suicide seems to be a silent epidemic. Li and Baker (1991) speculate that marriage problems and poverty may be the major causes of suicide for this group of women.
Croll (1978) points out that suicide had 1ong been an escape for women of all classes when their situation became unbearable and mentions statistics collected in the first two decades of this century showing that it was women in their early twenties who were most vulnerable. One of the reason why the Chinese government has remained so quiet about the suicide figures is that the social circumstances associated with suicide were supposed to be eliminated under socialism, or at least alleviated. These current figures suggest that this is not the case and that such behaviour is not a 'feudal remnant' but is clearly attributable to present conditions. Examples can easily be found in the 'one-child' policy, the preference for sons, female infanticide and ill treatment at the hands of husband and mother-in-law.
Suicide is, of course, not only a gesture of despair but may also be one of anger and revenge. This is particularly likely among a group who in other ways have so little control over their own lives, and little means of redress against the injustices they suffer. In destroying themselves, they also inflict damage on their persecutors. Many people still believe that the unquiet spirit of a suicide will return to haunt the household (Wolf, 1975). On the corporeal level, a suicide reflects very badly on the family and involves officials in an investigation, thus exposing family troubles to common scrutiny. In the routine life of a village, even with the advent of television, gossip about one's neighbours is a major form of entertainment and a suicide is guaranteed to get the village talking - a sweet revenge in such a 'face' conscious society.
WOMEN AND NEUROSIS
The Twelve Centre Epidemiological Survey found very low rates of neurotic disorder, defined to include hysteria, hypertension, anxiety, phobic conditions and depression (Xiang, 1986). Out of a total sample of 6952 people interviewed only 16 cases of neuroses in men and 134 in women were found. Xiang explains this by saying that Chinese doctors are diagnosing neurasthenia when faced with symptoms which Western doctors would identify as neurotic (Kleinman, 1986). The overall female rate is 39.93/1000 (urban 37.21/1000; rural 42.69/1000). The overall male rate is 4.71/1000 (urban 4.22/1000; rural 5.18/1000). If one accepts the level of neurotic disorder as a measure of distress, then women would appear to be more affected than men. However, a confounding factor is neurasthenia which is treated as a physiologically based disorder in China. We do not know whether doctors tend to diagnose neurasthenia more often in men (a physical disorder) and neurosis more frequently in women (a psychological disorder). If one looked at the combined figures for both these disorders a more equal pattern might emerge. Another possible factor may be that men experience distress in the same amounts as women but express it differently. Thus in an epidemiological study conducted in Hong Kong by Chen at al. (1993), the typical result was found with women experiencing neurotic anxiety and depression much more frequently than men. However, Chen et al. (somewhat unusually) included alcohol and gambling in their list of disorders. If one adds these to the male prevalence of anxiety and depression, the figure almost exactly equals that of women experiencing anxiety and depression. We need to know much more about the complex tapestry woven by the interaction between the biological, social and psychological in the subjective perception and expression of distress.
CONCLUSIONS
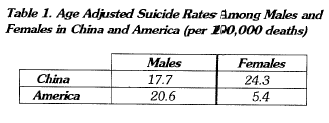
We can see from the material presented here that the mental health of women in China follows international patterns in some areas, for instance in their greater incidence of depression in comparison with men. In other areas, there is a significant departure from international norms. There are more completed female suicides in China, confounding one of the basic tenets in suicidology - that women are more likely to 'attempt' suicide, while men more frequently kill themselves. The most accurate figures currently available suggest that schizophrenia has a higher incidence among women than men, although it is probably wisest to accept that the full story has not yet unfolded in this area.
Whatever we know about the mental health of women in China has to be interpreted within a societal framework which remains significantly hostile to them. The government likes to argue that this atmosphere is generated by what they call 'the remnants of feudal attitudes' that must be combated but will eventually dissipate with time. This of course allows them to deflect responsibility onto 'the old society'. They are very reluctant to accept that while discrimination against women has, indeed, a very long history, what maintains it currently is not simply the old ways of thinking although these play a part, for instance in the strong preference for a son to carry on the family name. The goals of 'socialist spiritual civilization', particularly in economic areas, for which the government has to accept responsibility, are re-affirming women's inferior status. There is very much more freedom in China, at least culturally and economically, than there has been for many centuries. For someone who believes in both freedom and equality, it is a sad irony to have to accept that increased freedom has decreased equality.
REFERENCES
Aird J. S. (1990) Slaughter of the Innocents: Coercive Birth Control In China. American Enterprise Institute, Washington D.C.
Angermeyer M. C. and Kuhn L. (1988) Gender differences in age at onset of schizophrenia. European Archives of Psychiatry and Neurological Sciences 237: 351-364.
Banister, J. (1987) China's Changing Population. California: Stanford University Press.
Belle D. (1982) Introduction. In Lives In Stress: Women and Depression. (Ed. Belle D.) Sage, London.
Bemandez T. (1984) Prevalent disorders of women: attempts toward a different understanding and treatment. In Women and Mental Health: New Directions for Change. (Ed. Mowbray C. T., Lanir S. and Hulce M.) The Haworth Press, New York.
Braverman I. K., Braverman D. M., Clarkson D. E., Rosenkrantz P. S. and Vogel S. R. (1970) Sex role stereotypes and clinical judgements of mental health. Journal of Consulting and Clinical Psychology 34: 1-7.
Brown G. W. and Harris T. 0. (1978) Social Origins of Depression Tavistock, London.
Chen, C. N., Wong, J,, Lee, N., Chan-Ho, M. W., Lau, J., (1993) The Sha Tin community mental health survey in Hong Kong. Archives of General Psychiatry, 50:125-133.
Chen, C. H. (1986) Analysis of epidemiological data of schizophrenia. Chinese Journal of Neurology and Psychiatry 19, (2): 73-76, (in Chinese).
Cheung P. (1991) Adult psychiatric epidemiology in China in the 80s. Culture, Medicine and Psychiatry 15, 479-496.
Cooer, J. E. and Sartorius, N. (eds.) (1996) Mental Disorders in China Gaskell, London.
Co-ordinating' Group for the 12-Region Epidemiological Survey of Mental Illness (1996) An epidemiological investigation of mental disorders in twelve regions of China: methodology and data analysis. Chinese Journal of Neurology and Psychiatry 19, (2): 65-69 (in Chinese).
Co-ordinating Group for the 12-Region Epidemiological Survey of Mental illness (1986b) Investigation of the prevalence of various mental disorders and analysis of the data. Chinese Journal of Neurology and Psychiatry 19, (2): 80-82 {in Chinese).
Croll E. (1978) Feminism and Socialism In China. Routledge and Kegan Paul, London.
Goldstein J. M. (1988) Gender differences in the course of schizophrenia. American Journal of Psychiatry 145, (6): 684-689.
Kendall, R. E. (1988) Schizophrenia. In Companion to Psychiatric Studies. (Ed. Kendall R. E and Zealley A. K.) Churchill Livingstone, Edinburgh.
Kleinman A. (1986) Social Origins of Distress and Disease: Depression, Neurasthenia and Pain in Modem China. New Haven; Yale University Press
Leff J. (1986) Psychiatry Around the Globe. (2nd. ed.) Gaskell, London.
Li G. H. and Baker S. P. (1991) A comparison of injury death rates in China and the United States. American Journal of Public Health 81, (5): 605-609.
Lin K. M. (1981) Traditional Chinese medical beliefs and their relevance for mental illness and psychiatry. In Normal and Abnormal Behaviour in Chinese Societies (Edited by Kleinman. A. and Lin T. Y.) D. Reidel Publishing Company, Dordrecht.
Loranger A. W. (1984) Sex difference in age of onset of schizophrenia. Archives of General Psychiatry. 41: 57-161.
McGuffin P. and Katz R. (1989) The genetics of depression and manic-depressive disorder. British Journal of Psychiatry 155: 294-304.
Miles A. (1987) Women and Mental Illness: The Social Context of Female Neurosis. Wheatsheaf Books, Sussex.
Murray, C.J.L., Lopez, A.O. and Jamison, D.T., (1994) The global burden of disease in 1990; a summary of results, sensitivity analysis and future directions. Bulletin of the World Health Organization, 72, (3): 495-509.
Pearson V. (1995) Goods on which one loses: Women and mental health in China. Social Science and Medicine, 41, (8): 1159-1173.
Pearson V. (1995) Mental Health Care In China: State Policies, Professional Services and Family Respons ibilities Gaskell, London; American Psychiatric Press, New York.
Pearson, V. (1996) Women and health in China: anatomy, destiny and politics. Journal of Social Policy, 25, (4): 529-543.
Phillips M. R. et al. (1990) Issues Related to the Use of Assessment Instruments for Negative-Positive Psychiatric Symptoms. Science and Technology Press: Hubei (in Chinese).
Pritchard, C. (1996) Suicide in the People's Republic of China categorized by age and gender: evidence of the influence of culture on suicide. Acta Psychiatrica Scandanavica 93: 362-367.
Rosen S. (1987) Editor's introduction. Chinese Sociology and Anthropology XX (1): 5-12.
Sartorius N., Jablensky A., Korten G., Ernberg, G. Anker, M.,
Cooper J. E., and Day R. Early manifestations and first contact incidence of schizophrenia in different cultures. Psychological Medicine 16: 909-928.
Seeman M. V. (1982) Gender differences in schizophrenia. Canadian Journal of Psychiatry. 27: 107-111.
Torrey E. F. (1988) Surviving Schizophrenia: A Family Manual Harper and Row, New York.
Tseng W. S. (1973) The development of psychiatric concepts in traditional Chinese medicine. Archives of General Psychiatry 29, (4): 569-577.
Wolf M. (1975) Women and Suicide in China. In Women in Chinese Society. (Ed. Wolf , M. and Witke, R.) Stanford University Press, California.
World Bank (1989) World Development Report. The World Bank, Washington, DC
World Bank (1992) China: Long Term Issues and Options in the Health Transition. The World Bank, Washington, DC.
Xiang M. (1986) An epidemiological investigation of neurosis in 12 districts of China. Chinese Journal of Neurology and Psychiatry 19 (2): 87-91.
Yan S. M. and Xiang D. H. (1984) Psychiatric care in the People's Republic of China. IRCS Medical Science-Biochemistry 12, (3): 193-194.
Yuan T. G. (1987) The transformation of the schizophrenic subtype in the last twenty years. Chinese Journal of Neurology and Psychiatry 20, (6): 340-343 (in Chinese).
Zeng, Y., Tu P., Gu, B. C., Xu, Y., Li, B. H. and Li, Y. P. (1993) Causes and implications of the recent increase in the reported sex ratio at birth in China. Population Development Review 19,(2): 283-302.
Zhao Y. Z. (1986) The analysis of epidemiological data of psychosis other than schizophrenia. Chinese Journal of Neurology and Psychiatry. 19, (2): 77-79 (in Chinese).
Veronica Pearson BSc(Econ), MSc, CQSW, DPhil Professor, Department of Social Work and Social Administration, The University of Hong Kong, Pokfulam Road, Hong Kong.
