
Hong Kong Journal of Psychiatry (1999) 9 (1) 12-14
ORIGINAL ARTICLE
Summary
A survey of the prevalence of dementia among elderly was conducted in three different areas of Shanghai , the People’s Republic of China. The DSMI- III- R was used as diagnostic criteria. The prevalence of dementia in the whole sample was 4.21%: Alzheimer’s disease (3.15%) and vascular dementia (0.85%). The prevalence increased with age: 1.78% among those aged 60-64, 3.9% among 70-74, 12.45% among 80 years and older. The prevalence was higher in women and in urban residents. The potential risk factors of dementia were formulated and discussed.
Key words: prevalence, senile dementia, Chinese
INTRODUCTION
In developed countries, the prevalence of severe dementia among persons aged 65 years and older has been estimated to be between 1.3% and 6.2%, with an average rate of about 4.5%. The prevalence of mild dementia has been reported to vary from 2.6% to 10.8%. The prevalence of dementia, mild and severe, was between 6.6% and 15.8% (Mortiner, et al. 1981; Shahavama, et al. 1986; Garland & Cross, 1982; Mortiner, 1983). In China, there have been limited epidemiological investigations on dementia among elderly. Previous papers have shown that among the aged population, 0.46% to 1.86% had dementia and the prevalence of Alzheimer's disease (AD) was between 0.07% to 0.66% (Chen, et al. 1987; Kuang & Zhao, 198l;Yan & Liu, 1988). We had conducted an epidemiology study of dementia among elderly in Shanghai and nearby areas from October to December 1990. Three research units collaborated in the survey: Shanghai Mental Health Center, Shanghai Jiading County Mental Health Center, and Shanghai Zabei Dismct Mental Health Center.
METHODS
The Mini-Mental State Examination (MMSE) (Folstein, et al. 1975), a brief screening tool with high validity, sensitivity and specialty, was used. The cut-off points used to identify probable cases of dementia were 17 for subjects with no education, 20 for elementary education, and 24 for those who received primary middle or above education respectively (Wang, et al 1989).
CASE SCREENING:
Twenty healthy elderly people were rated with MMSE by 14 psychiatrists. The concordance rate was 0.95. A stratified radom sampling method was used in a country, a town and a suburban area. A cohort of 4597 subjects aged 60 or above was investigated. 3779 subjects were interviewed by investigators. 1499 were male and 2280 were female (M:F=l:1.57). 1219 of them lived in urban district, 2045 lived in rural area and 515 in suburban area.
DIAGNOSIS MAKING
The elderly individuals scored lower than the cut-off points on MMSE were interviewed by 2 investigators. The diagnosis of senile dementia or Alzheimer's disease was made according to the DSM-HI-R criteria (American Psychiatric Association, 1986). Hachinski Ischemic Scale (1-IlS) (Hachinski, 1978) was also used. From those 316 individuals scored higher than the cut-off points, about 10% were found meeting the criteria of dementia.
RESULTS
THE PREVALENCE OF DEMENTIA
One hundred and fifty nine subjects met the DSM-III-R criteria of dementia. Seventy of them lived in city, 80 in countryside and 8 in small town. The prevalence of dementia in the city, countryside and small town were 5.74%, 3.90% and 1.55% respectively. There was statistically significant difference among the three areas (X2=11.42, P<0.001).
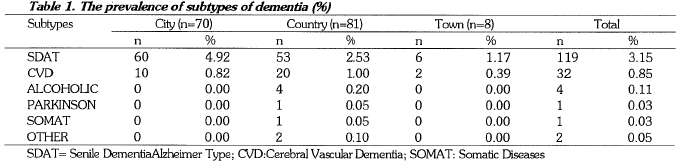
SUBTYPES OF DEMENTIA
The prevalence of senile dementia Alzheimer type (SDAT) in city was 1.9 times and 4.2 times of that in countryside and town (table 1), while the figures of cerebrovascular dementia (CVD) were similar in city and countryside, but were higher than that in town.
SEX, AGE AND DEMENTIA
Among the 159 demented patients, 24 were male, 135 were female (Male:Female=l:5.6). The prevalence of dementia among male and female are 1.60% and 5.92% respectively, and there was statistically significant difference between them (X2=40.96, P<0.001). As regard to the urban area, the prevalence among male vs. female were 1.2% vs. 8.44%, while those in rural and suburban area were 2.26% vs. 5.04% and 0.00% vs. 2.89% respectively. On the other hand, the prevalence of SDAT in male and female were 1.33% and 4.34% respectively, there was significant difference between them (P<0.05).
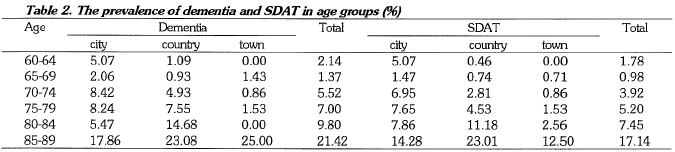
The patients' ages ranged from 60 to 87 years (mean+/SD=5.00+/- 8.00). There was no significant difference between city (74.00 +/- 7.00 yrs) and countryside (77.00 +/- 7.00 yrs), but there was between city and town (table 2).
For the demented patients, except for the group aged 65-69, whose prevalence was lower than those aged 60-64, the prevalence generally increased with age. Among those above 75 years, the prevalence varied from 1.37% to 7.00%, but among those who were older than 80 years, the figures we.re between 9.80% to 21.42%. The prevalence of SDAT increased significantly in subjects who were 75 years and above and was varied from 7.45% to 17.14% with the highest prevalence in rural area.
EDUCATION LEVELS AND DEMENTIA
The prevalence of dementia among the elderly with different educational levels were 4.77% for those who had no education, 3.68% for those with elementary and 3.58% for subjects with primary middle education. The prevalence were significantly higher than those who were educated to senior middle (2.14%) or college (1.33%) levels. With regard to SDAT, the prevalence among those with no education (4.66%) was about 4 times higher than the other four groups (1.30% to 1.54%).
SEVERITY OF DEMENTIA
Ninety-nine of 159 (62.26%) demented elderly were diagnosed as mild, 49 (30.81%) as moderate, and 11 (6.92%) as severe. The prevalence rates of mild dementia in city, countryside and small town were 4.90%, 1.00% and 2.20% respectively; which were higher than the moderate ones (1.55%, 0.20% and 1.51% respectively) and the severe ones (0.16%, 1.00% and 0.24% respectively). The results also showed that the mild dementia in urban area was 5 times as much as that in rural area, and 2 times as that in suburban area. It needed further research to explain this phenomena. From our viewpoint, it may be due to that most of the illiterates living in the countryside, they might account for more lost cases getting lower scores than cut-off points on MMSE.
THE MORBIDITY OF SDAT AND CVD
In 1986, the morbidity of SDAT at Zabei disbict and Jiading county were 0.33% and 0.21% respectively, while CVD at these two areas were 0.15% and 0.19% respectively. Table 3 shows from then on, that the morbidity of SDAT have decreased yearly, especially in the countryside. However, the CVD have increased within the same duration. In addition to this, the mean morbidity of SDAT was 1.6 times as that of CVD. The ratios of SDAT vs. CVD were 1:2.2 for urban area and 1:1.1 for rural area.
DISCUSSION
With difference in sample size, methodology and diagnostic criteria, the previous reports on prevalence of dementia varied among different studies: 4.00% to 5.00% in Europe and USA (50% SDA1), 4.00% in pre-Soviet countries (1.60% SDA1) and 4.50% to 4.70% in Japan (0.07% - 4.70% SDA1) (Yan & Liu, 1988). The rates in China were reported between 0.46% to 1.80% (0.07% - 4.36% SDA1) (Yan & Liu, 1988; Folstein, et al. 1975; Wang, et al. 1989; American Psychiatric Association, 1986). In the present ·survey, the prevalence of dementia among elderly is 4.21%, while SDAT accounts for 3.15%. The result is similar to previous studies. For getting more comparable and reliable results, a more concordant research method among different researchers should be recommended. SDAT has been found in our study to be the commonest subtype of dementia (account for 74.80%), which followed by CVD (20.1%). This result is also similar with those of European's and American's (Kuang & Zhao, 1981), but differ with that of Japanese's in which the CVD was much more than SDAT (Yan & Lu, 1988). Although brain imaging techniques were not used in our study, we believed that the false negative diagnosis of CVD is minimized by using the HIS as the tool of identification. However, we will take the Japanese report into account since it has been found from our study that the morbidity of CVD has the tendency of rising yearly.
The present investigation indicates that the prevalence of dementia among female is 3.7 times higher than that of male. This is similar to the findings from Zhang et al (1990). It might be due to longer life span and lower educational level of women than men. On the other hand, the prevalence of dementia in the group aged 80-84 years is 3.75 times higher than those aged below 75-79 years, and for SDAT, the figure is 3.81. It is similar with other articles.
The prevalence of dementia in city is 1.45 and 3.70 times higher respectively as compared with those lived in countryside and town, while the prevalence among illiterates is 2 to 4 times higher than those education with middle school or above. This indicates that some variables such as female, aged above 80 years, and lower educational level may be the risk factors for predicting the morbidity of dementia.
When we examined the individuals scored higher than the cut-off points on the MMSE, 2 .21% of them were diagnosed as dementia. This mild higher rate may be related to the cut-off points themselves. Since some differences such as various actual learning duration in the school, the physical and psychological variations between illiterates and those educated people, etc., have not been completely included into the MMSE. So that the cut-off points on MMSE are limited in reflecting the concordance of educational levels. Thus, the further revised rating scales which aimed to settle the above difficulties should possibly reduce the items immediately depending on educational levels not only by their quantity, but also by their constructional ratio in total.

REFERENCES
American Psychiatric Association (1986) DSM-III-R. Washington DC; APA, 1986:4
Chen X.S., Zhang J.Z., Jiang Z.N. (1987) A psychiatric epidemiological survey on elderly in Beijing city. Chinese Journal of Neurology and Psychiatry, 11: 89-92.
Folestein M.F., Folstein S.E., McHugh P.R. (1975) Mini-Mental State Examination, a practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12: 189.
Garland B.J., Cross P.S. (1982) Epidemiology of psychopathology in old age. Psychiatric Clinic of North America, 5: 11-26.
Hachinski V.C. (1978) Cerebral blood flow differentiation of Alzheimer's disease from multifarct dementia. In: Alzheimer's disease, senile dementia and relation disorder (Vol. 7) (edited by Katman R., Terry R.D., Bick K L.). New York, Raven Press, 97-102.
Kuang P.G., Zhao C.D. (1981) A sampling survey of geriatric mental disturbances at Wuhan in 1981. Chinese Journal of Neurology and Psychiatry, 19: 145-148.
Mortiner T.A., Schamm L.M., Fench L.M. (1981) Epedimiology of dementing illness. In: The epidemiology of dementia. New York, Oxford Unviersity Press.
Mortiner T.A. (1983) Alzheimer's disease and senile dementia: prevalence and incidence. In: Alzheimer's disease (edited by Reisberg B.) New York, Free Press ,144-148.
Shahavama H., Kasahara H., Kobayashi H. (1986) Prevalence of dementia in a Japanese eldrly population. Acta Psychiat.ric Scandinavia, 74: 144-145.
Wang Z.Y., Zhang M.Y., Qu G.Y., (1989) The application of MMSE (Chinese version). Archives of Psychiatry (Shanghai, China),7: 108-110.
Yan T.S., Lu Y.X. (1988) A survey of physical and mental health among 1229 elderly over 65. Chinese Journal of Neurological System and Mental Disorders, 14: 85-87.
Zhang M.Z., Katzman R., Solomon D. (1990) The prevalence of dementia and AD in Shanghai, China: impact of age, gender, and education. Annual Neurology, 27: 428-437.
Gao ZX M.D, Professor of Psychiatry, Department of Geriatric Psychiatry, Shanghai Mental Health Center;
Fang YS M.D, Psychiatrist, Shanghai Mental Health Center; Xie B M.D, Psychiatrist, Shanghai Mental Health Center;
Pan JX M.D, Psychiatrist, Jiading County Mental Health Center, Shanghai
*Correspondence: Dr. Gao Z.X., Shanghai Mental Health Center, 600 Wan Pin Nan Road, 200030, Shanghai, PR China
