
Hong Kong J Psychiatry 2004;14(4):15-23
ORIGINAL ARTICLE
S Gandotra, SE Paul
Dr Sachin Gandotra, DPM, Senior Resident, Central Institute of Psychiatry, Kanke, Ranchi, Jharkhand, India
Dr SE Paul, MD, Oxford House, London Road, Bishop's Stortford, Hertfordshire, UK.
Address for correspondence: Dr Sachin Gandotra, Room No. 36, Men's Hostel No. 2, Central Institute of Psychiatry, Kanke, Ranchi 834006, Jharkhand, India.
E-mail: sachincip@rediffmail.com
Submitted: 8 September 2004; Accepted:14 February 2005
Abstract
Objective: Akiskal's view that a temperamental proneness lies in the roots of bipolarity has adequate empirical support from extensive clinical studies. This study was designed to investigate the relationship between affective temperaments and outcome in terms of polarity in bipolar I illness and to assess socio-occupational functioning in patients with these temperaments.
Patients and Methods: 102 outpatients and inpatients meeting the Diagnostic and Statistical Manual of Mental Disorders-IV criteria for bipolar I disorder were recruited from consecutive patients admitted to hospital. Patients were evaluated when in a euthymic state using the Mont- gomery-Asberg Depression Rating Scale or the Bech-Refaelson Mania Rating Scale. The crite- ria developed by Akiskal and Mallya were used to assess the hyperthymic, depressive, cyclothymic, and irritable temperaments in a dimensional approach. The Socio-Occupational Functioning Assessment Scale was used to assess socio-occupational functioning.
Results: Regression analysis indicated that the total number of episodes (manic and depressive) was significantly associated with the depressive score. Further, the total number of previous depressive episodes positively correlated with the depressive score and negatively correlated with the hyperthymic score. Patients who had had a recent manic episode had a hyperthymic score, while those who had the most recent depressive episode scored high on the depressive score. A significant impairment in socio-occupational functioning in patients with a depressive temperament was noted.
Conclusions: These findings agree with the hypothesis that affective temperaments represent a putative stage in the clinical evolution of bipolar illness and reflect a trait-state continuum be- tween temperaments and affective episodes. Patients with depression were significantly im- paired in their socio-occupational functioning.
Key words: Affective disorders, Bipolar disorder, Treatment outcome
Introduction
Temperament classically refers to an adaptive mixture of traits that can lead to illness or modify the expression of superimposed affective states.1 Hippocrates propounded the view that small excesses of essential humours and blood produced phlegmatic, choleric, and sanguine personalities. This was the first attempt to explain differences in temperaments and personalities. In the second century, Arateus observed the connection between melancholia and mania.2 The historic roots of dysthymic and cyclothymic disorders as part of the subaffective spectrum are essentially Greek. Kraepelin considered affective temperaments as life-long attenuated, subclinical forms of manic-depressive psychosis, with a trait-state continuum.3,4 Kretschmer postulated a continuum between the cyclothymic character and manic- depressive psychosis.5 The work of Schneider extended Kraepelin's observations and led to descriptions of the depressive and hypomanic types, which are the 2 basic temperaments in the Kraepelinian scheme.6
Akiskal et al began to revitalise Kraepelin's concept of fundamental states, which these researchers regarded as the temperamental basis of affective illness.7 Akiskal pro- posed temperamental dysregulation as the developmental substrates from which affective episodes arise, thereby delineating temperamental pathways to bipolarity.8 More recently, some authors have suggested that one of the major points of interest with temperament is its ability to explore the clinical and predictive significance of sub-affective traits and inter-episodic manifestations of recurrent mood disorders within a spectrum of bipolar illness.9-16 The main evidence linking hyperthymia to the bipolar spectrum has come from the use of family history as an external validator:17 patients with major depression who exhibited at least 5 of 7 hyperthymic attributes had significantly higher rates of familial bipolarity than patients with strictly unipolar disorder without these temperamental attributes and who, from a familial perspective, were indistinguishable from patients with bipolar II disorder. Hyperthymia also appears to be relevant to the course of manic and depressive states.18-20 When hyperthymia occurs in association with mania, the latter often pursues a recurrent course. However, when hyperthymic traits precede depressive states, they tend to colour the depression with 'mixed' (hypomanic) features.
The French national multi-site collaborative study on the clinical epidemiology of mania (EPIMAN study) re- vealed an important finding that patients with mixed mania had a higher percentage of depressive temperamental traits compared with those with pure mania,18 thereby supporting Akiskal's hypothesis that mixed states are best conceived as a reversal of temperament to its episode of opposite polarity.21,22 In other words, dysphoric mania arises from the intrusion of a depressive temperament into a manic episode, or when mania is superimposed on a depressive temperament.
Cassano et al showed that, in patients with unipolar disorder with hyperthymic temperament, family history and sex distribution have a closer association to those of bipolar I and II disorders rather than to pure unipolar disorder without hyperthymic temperament.23 The fact that at least 10% of patients with major depression in an Italian study could be characterised as premorbidly hyperthymic suggested that this temperament has relevance to both major affective poles.24
Other studies have focused on the fact that temperaments may broaden the spectrum of bipolar disorders. This broad- ening may provide one solution to the competing needs between the clinical and research worlds. Specifically, by identifying subgroups of patients within a broader definition, researchers have a narrower patient population to permit more homogeneous samples, while the clinician has a broader umbrella to permit a starting point for treatment development.
A search of the literature did not yield any study that investigated the relationship between the 4 affective tem- peraments of hyperthymic, depressive, cyclothymic, and irritable, and the main characteristics of bipolar illness. This study aims to explore the impact of temperament on the evolution of bipolar illness. Further, outcome in terms of socio-occupational functioning of the patients was assessed. There has been a relative lack of such research in the Indian context. Assessment of such subaffective traits could have significant consequences for their clinical and predictive importance.
Patients and Methods
102 patients meeting the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) criteria for bipolar I disorder who were followed up in the outpatient department or admitted as inpatients to the Central Institute of Psychiatry, Ranchi, India, during an 8-month period were enrolled in the study. The patients were aged between 18 and 60 years. Informed consent was obtained from each patient. Patients with any comorbid psychiatric condition including substance dependence, history of any head injury or seizure disorder, or serious medical disorder requiring treatment were excluded from the study.
The study was a cross sectional hospital-based study. The patients were confirmed to be clinically euthymic when included in the study by means of the Montgomery-Asberg Depression Rating Scale (MADRS)25 or the Bech-Refaelson Mania Rating Scale (BRMAS),26 depending on when the most recent episode occurred. To study the effect of the most recent episode of bipolar I illness on the patients' tem- perament, patients in remission were analysed separately. Remission was defined as 2 symptom-free months following an episode, according to the DSM-IV criteria for remission in affective disorders.
To evaluate the temperaments, the Semi-Structured Affective Temperament Interview (SSATI)27 was applied. The SSATI consists of 32 items covering the 4 tempera- ment traits — 7 for hyperthymic temperament, 7 for depressive, 8 for irritable, and 10 for cyclothymic. The in- ternal consistency coefficient for the 4 scales was very high (Cronbach's a = 0.85, 0.86, 0.94, and 0.88 for the depressive, hyperthymic, cyclothymic, and irritable temperamental scales, respectively).28 The SSATI was used to assess affec- tive temperaments because commonly used temperament instruments as the Eysenck Personality Inventory,29 derived from experimental psychology, are not routinely used in psychiatric practice. Likewise, the more recent contribution to the study of personality and temperament by Cloninger et al30 does not use explicit affective terminology.
For the purpose of the study, the criteria of Akiskal and Mallya27 for affective temperaments were translated from English into Hindi from English by 5 translators who did not know the Hindi version of the criteria. The Hindi versions were back-translated into English by another group of 5 translators, and the translation was checked for conformity. Finally, a bilingual native English speaker, who had confirmed the original meaning of the items, checked the accuracy of the translation and its conformity with the original version. A conscious effort was made to ensure conceptual, semantic, and technical equivalency between the source measures and the target measures. During the preparation for the study, the interviewers were trained to reliably read out the items of the interview in the locally spoken Hindi dialect and rate the responses accordingly. As a result, there was substantial inter-rater agreement on the items of the interview. The question format of the original criteria was retained. The items were randomised for this study to avoid the possibility that patients may respond in the same way to all subsequent questions on a given scale. At the start of the interview, each patient was instructed to answer by considering his/her habitual self extending as far back as he/she remembered. In addition, at a random juncture in the interview, patients were asked to confirm that their responses pertained to attributes that began in- sidiously at an early age. Temperamental characteristics were considered to be a dimension rather than a category, thus avoiding arbitrary thresholds in the constitution of categories.
The Socio-Occupational Functional Assessment Scale (SOFAS)31 was used to assess the socio-occupational functioning of the patients. The SOFAS, which has been proposed as a new axis in Appendix B of the DSM-IV, focuses only on functioning and not on symptoms and does not try to discriminate between functional changes related to psychiatric and non-psychiatric causes. The scale is a clinician-rated 100-point scale based on all available information, with clear descriptions of each 10-point interval. Ratings are generally made for the past week, but longer intervals (e.g., highest during the past year) can be used. Instructions for rating the SOFAS are included in the DSM-IV; clinician raters do not require additional train- ing to use the scale. The scale considers socio-occupational functioning on a continuum from excellent functioning to grossly impaired functioning and includes impairments in functioning due to physical limitations, as well as due to mental impairments. To be counted, impairment must be a direct consequence of mental and physical health problems; the effects of lack of opportunity and other environmental limitations are not considered.
Statistical Analysis
The patients were divided into 4 categories on the basis of their temperamental scores, and the impact of temperamen- tal status differences on the outcome for bipolar I disorder was analysed using the Statistical Package for the Social Sciences version 10.0. Log transformations were made to remove skewness, when appropriate. Log transformation of each total temperamental score was done, and association between continuous variables and temperament dimensions was carried out using linear correlation. Categorical variables were assessed using 1-way analysis of variance (ANOVA) and the independent samples t test, depending on the num- ber of categories. Regression analyses were done to assess the contribution of the temperamental status to the outcome for bipolar I illness. The relationship between continuous variables and temperament dimensions was done using linear regression. Logistic regression, both bivariate and multinomial, was done for categorical variables, depending on the number of categories.
Results
The mean (standard deviation) age of the patients was 30.65 ± 9.51 years. There were more men (70; 68.6%) than women (32; 31.4%). A similar pattern was found for marital status, with 72 patients (70.6%) being married and 30 patients (29. 4%) being single. The mean age at the onset of the first episode was 22.18 ± 7.41 years. The proportion of patients with bipolar disorder for whom the onset of illness was a manic episode was 93 (91.2%), and 8 patients (7.8%) had a depressive onset; only 1 patient (1.0%) had mixed-episode onset. The mean number of anamnestic episodes was 3.45 ± 2.21, the number of previous manic episodes was 2.04 ± 1.80, and the number of previous depressive episodes was 0.4 ± 1.15. Forty six patients (45.1%) had a most recent manic episode, while 20 patients (19.6%) had a most recent manic episode in full remission.
Similarly, 12 patients (11.8%) had a most recent depres- sive episode and 6 patients (5.9%) had a most recent de- pressive episode in full remission. Thirteen patients (12.7%) had had a single manic episode. The mean duration of the illness was found to be 93.50 ± 92.94 months. Only 1 pa- tient (1.0%) had attempted to commit suicide during the illness. Thirty eight patients (37.3%) had a family history of affective illness, 9 (8.8%) had a family history of other psychiatric illnesses, including all psychiatric illnesses ex- cept for affective illness, and 4 (4.0%) had a family history of affective illness as well as other psychiatric illnesses; 51 patients (50.0%) had no contributory family history.
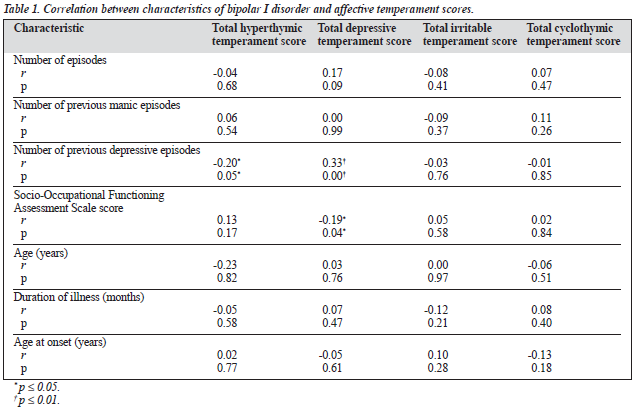
Table 1 shows the correlation between various charac- teristics of illness and the affective temperament scores. It is clear that there was a significant positive correlation be- tween the number of previous depressive episodes and the depressive temperament score (p < 0.005), while there was a significant negative correlation between the number of previous depressive episodes and total hyperthymic tempera- ment score (p = 0.05). This trend was also observed after linear regression analysis. There was also a negative corre- lation between the SOFAS score and the total depressive temperament score (p < 0.05), indicating that patients with a depressive temperament were more socio-occupationally impaired than patients with other temperament types. The relationships between variables such as type of first episode, family type, and family history and the affective tempera- ment score were evaluated using ANOVA. No significant association was found between these variables and the affective temperament score.
Regarding the occurrence of the most recent episode, a statistically significant association was found between the total depressive temperament score and those patients with the most recent manic episode in full remission (p < 0.01) [Table 2]. Thus, those patients with the most recent manic episode scored low on total depressive temperament items in the semi-structured interview. Similar trends were observed between those patients with the most recent depressive episode and those with a single manic episode. The patients with recent depressive episode had a statisti- cally significant association with total hyperthymic tempera- ment score (p < 0.001) and depressive temperament score (p < 0.05). Similarly, an association between the total depressive temperament score and a single manic episode also reached statistical significance (p = 0.005). The patients were divided into 2 subgroups of those with the most recent manic episode and those with the most recent depressive episode to provide greater samples in either category for a more reliable result and a group comparison was done with the affective temperaments. Patients with recent depressive episode had a significantly higher depressive temperament score (p = 0.005), while those with recent manic episode had a significantly higher hyperthymic temperament score (p < 0.001) [Table 2]. Women with bipolar I disorder were more likely to have a depressive temperament (p < 0.01) and men with bipolar I disorder had a tendency towards a hyperthymic temperament (p < 0.05).
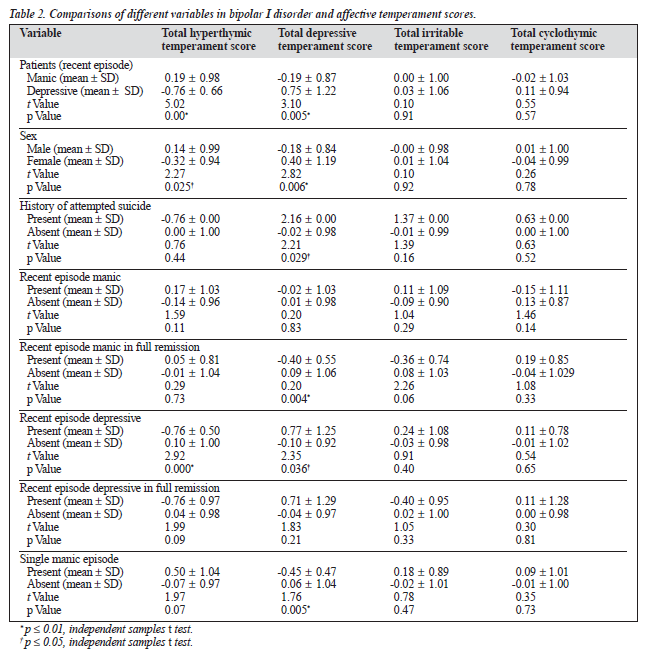
The history of suicide attempts was influenced by tem- perament status since there was a significant association between depressive temperament scores and attempted suicide (p < 0.05) [Table 2]. However, this finding needs to be treated with caution since the sample had only 1 patient who attempted suicide.
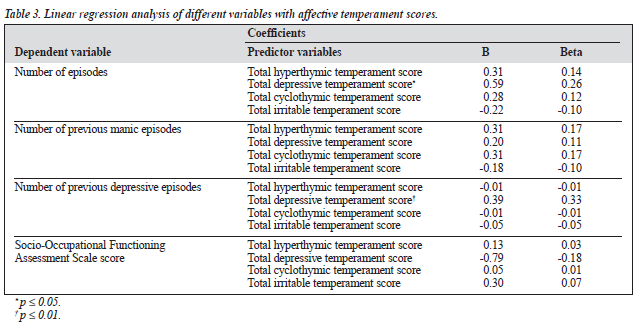
Regression analysis was done to assess the contribution of the affective temperament scores to the evolution of the bipolar I illness. Linear regression analysis, as indicated in Table 3, shows that the total number of episodes (manic and depressive) was positively correlated with the depressive temperament score (B = 0.599; p < 0.05). The total number of previous depressive episodes was significantly correlated with the total depressive temperament score (B = 0.394; p < 0.01). Therefore, patients with depressive temperament are more likely to have more depressive episodes than manic episodes. Conversely, the presence of hyperthymic temperament was associated with fewer depressive episodes. Thus, a depressive temperament may be considered predictive for an increased frequency of episodes, and for a depressive polarity of these episodes.
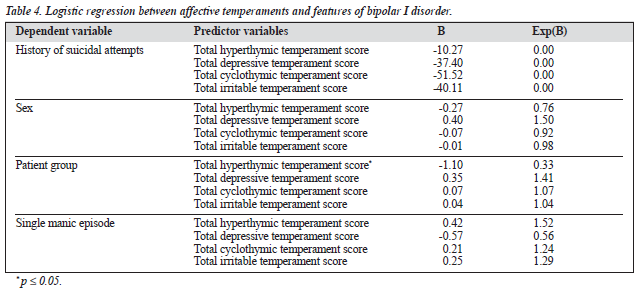
This association is further strengthened by regression analysis, as shown in Table 4. There was a significant negative correlation between the most recent episode in either of the patient groups (manic and depressive) and the hyperthymic temperament score (B = -1.103; p < 0.05).
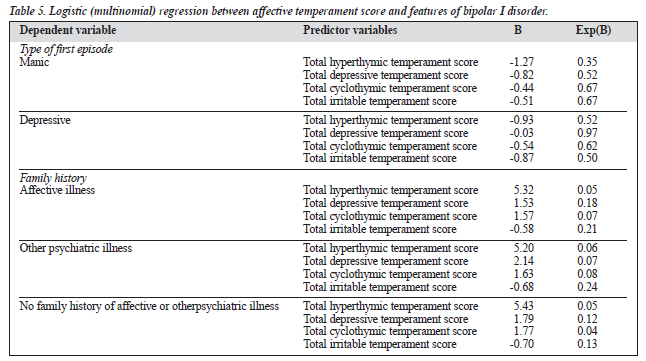
Although initial statistical analysis revealed significant associations between affective temperaments and charac- teristics of illness such as suicide attempts and sex, the affec- tive temperaments were not found to predict the outcome of bipolar I disorder in logistic regression analysis (Table 4). No association was found between the affective tempera- ments and other variables assessed such as duration of illness and age of onset of illness. Regression analysis also revealed that affective temperaments may not predict socio-occupational impairment. As is evident from Table 5, multinomial regression revealed no relationship between the affective temperaments and such variables as type of first episode and family history.
Discussion
Assessment of temperaments was carried out when patients had achieved remission, confirmed by low scores on the MADRS and BRMAS. It is therefore unlikely that the present findings may be explained by state-dependent variables. Klein showed longitudinal stability and a lack of thymic state-dependency with the depressive temperament.32 In the present study, an interesting observation was that, despite low scores on the MADRS and BRMAS, patients' temperament appeared to be coloured by their illness. This was greatest for patients with the most recent depressive episode. To ameliorate potential bias, only a few patients in full remission were assessed. The colouring of the tempera- ments was somewhat reduced, but reminiscences of the episode were noted to occur, and repeated attempts were made during the interview to encourage the patients to answer the questions as their habitual selves as far as they remembered. The observations of this study are consistent with those of Akiskal, who suggested that the state depen- dency of most personality measures is well documented and, in patients with chronic or sub-threshold mood disorders, personality maladjustment is best considered to be post- affective, arising from the distortions and conflicts that affective disturbances produce in the patient's life.33,34
There is now evidence that bipolar temperaments, either depressive or manic, colour the acute episode.19,20,28,35 It is also possible to differentiate 2 subtypes of bipolar I disorder: a subtype "with a predominance of manic psycho- pathology";36 and "prevailing depressed",36 "depression prone",37 or "poor prognosis subtype marked by a relative persistence of depressive symptoms".38 More research is required to determine the best choice of treatment for these subcategories, especially for the choice of mood stabilisers and antidepressants.
This provokes curiosity as to whether the affective temperaments precede or follow the episodes of the illness. At present, no definitive conclusions are available.24 However, indirect evidence supports the hypothesis that temperamental attributes develop early in life and determine the long-term functioning of the individual.39 Studies of patients and volunteer populations have shown that these attributes often exist without the occurrence of major affective episodes. Finally, the major depressive group in the Pisa-Memphis study included patients with both depressive and hyperthymic temperaments;40 the authors suggest that if temperament was simply a postepisodic attribute or if its evaluation merely reflected state effects of depression, they should not have found any hyperthymic attributes in the major depressive group. As noted earlier by Kraepelin, temperament shades gradually into normal variation.3 However, temperament may provide the physiological substrate on which other aspects of bipolar disorder are potentially imposed. The specificity of the relationship between temperament and other aspects of bipolar disorder is also not yet understood. For example, temperament may be something that interacts with bipolar disorder, but is inherited independently. Alternatively, temperament may represent a useful indi- cator of genetic predisposition.41
This study considered temperaments as dimensions rather than categories. The main advantage of this approach is that it avoids the researchers establishing any arbitrary thresholds in the constitution of categories. Although this approach has not been frequently used in previous studies, the study by Henry et al assessed the impact of depressive and hyperthymic temperaments on the outcome of bipolar illness while considering these temperaments as dimensions.20
In this study, it was shown that a high score for de- pressive temperament is associated with a greater lifetime number of episodes, and also of a depressive polarity. Further, the elevation in the hyperthymic temperament score is associated with a reduced number of depressive episodes. Thus, this study shows a continuum between temperament and polarity of episodes. These results are consistent with previously reported data. Henry et al,20 in their study of 72 patients with bipolar I disorder, found that a high score for depressive temperament was associated with a greater life- time number of episodes and a higher percentage of major depressive episodes than a low score.20 Conversely, a high hyperthymic score was associated with a strong trend to have manic rather than depressive episodes. The present study did not reveal such an association between the hyperthymic temperament score and the number of manic episodes, but it did show that patients with an elevated total hyperthymic score were less likely to have depressive episodes.
This study also showed that the most recent episode, either manic or depressive, was significantly associated with the temperamental status. Patients with recent manic episode scored high on the hyperthymic temperament score, while those with the most recent depressive episode scored high on the depressive temperament score. Kraepelin4 observed that affective temperaments occurred in the premorbid histories of most of the manic-depressive proband who returned to their basic temperament rather than to normality when in remission.4 Later studies have tried to explore the temperaments in terms of clinical and predictive significance of subaffective traits and interepisodic manifestations of recurrent mood-disorders within a spec- trum of bipolar illness.13,14,35 Hyperthymic temperament as a dimension is quite common among adolescents and young adults and these characteristics probably reflect over- adaptive, genotypically selected temperamental traits whose phenotypic expression has been favoured by environmental conditions. The present study revealed that hyperthymic characteristics were more frequent in men than in women, while depressive characteristics were more frequent in women than in men. This is consistent with findings reported in the literature.40,42 Only in Klein et al's study10 did adoles- cent females obtain a significantly higher score on the self-rating Hypomanic Personality Scale of Eckbald and Chapman.43
History of suicide attempts was found to be influenced by the depressive temperament status. However, this find- ing should be viewed with caution as a single patient in the study group had attempted suicide. Henry et al observed a similar finding in their study.20 Using the Temperament and Character Inventory, Cloninger et al found a strong association between melancholy and suicide attempts.44 These researchers found consistent relationships between suicide attempts and low cooperativeness and self- directedness. Patients with cyclothymic temperaments, with low self-directedness but high cooperativeness, often experienced depression but were not more likely than a healthy person to attempt suicide. Autocrats, who are high in self-directedness but low in cooperativeness, were hostile towards others but unlikely to attempt suicide. Thus, individuals with personality traits characterised by both low self-directedness and low cooperativeness are at increased risk of both attempted and completed suicide.44-47
This study showed a significant impairment in socio- occupational functioning in patients with depressive temperament. In a recent study, persistence of depressive symptoms in patients with bipolar I disorder in the first 2 years correlated with impairment after 15 years in areas such as household duties, recreational activities, overall satisfaction, and global social adjustment, and this predicted poor prognosis of this bipolar subtype.48
The limitations of the present study were that the as- sessed temperaments seemed to be coloured by their most recent episode despite efforts to assess the temperaments when the patients were in complete remission. A larger sample of patients in full remission possibly could have settled the bias. Further, the depressed population was under-represented.
Future studies should consider investigating comorbidity, phenomenology, treatment response, and assessment of temperament in relatives to strengthen the hypothesis of the trait-state continuum between personality and affective episodes, which could represent expression of the same genetic or constitutional endowment.
Depressive temperament can be considered predictive for an increased frequency of episodes, and for a depressive polarity of these episodes. Patients' affective temperament also appears to influence outcome in terms of the most recent episode of illness — that is, patients with a recent manic episode score high on hyperthymic temperament and those with a recent depressive episode score high on de- pressive temperament. These findings show that affective temperaments represent a putative stage in the clinical evo- lution of bipolar illness and reflect a trait-state continuum between temperament and affective episodes
References
- Akiskal HS. The temperamental foundations of mood disorders. In: affective disorders. London: Gaskel; 1996:3-30.
- Aretaeus of Cappadocia. In: Adams F, editor. The extant works of Aretaeus, the Cappadocian. London: Sydenham Society. Cited by: Akiskal HS. Mood disorders: clinical features. In: Sadock BJ, Sadock VA, editors. Comprehensive textbook of psychiatry. Vol 1. 7th ed. Baltimore: Williams and Wilkins; 2000:1169-1198.
- Kraepelin E. Die Erscheinungsformen des Irreseins. Z Gesamte. Neurol Psychiatr 1920;62:1-29. Cited in: Hirsch SR, Shepherd M, editors. Themes and variations in European psychiatry. Bristol: Wright; 1974; 7-30.
- Kraepelin E. Fundamental states. In: Robertson GM, editor. Manic de- pressive insanity and paranoia. Edinburgh: Livingstone; 1921:117-132.
- Kretschmer E. Physique and character. London: Kegan Paul; 1936
- Schneider K. Psychopathic personalities. London: Cassel; 1958.
- Akiskal HS, Djenderedjian AH, Rosenthal RH, Khani MK. Cyclothy- mic disorder: validating criteria for inclusion in the bipolar affective group. Am J Psychiatry 1977;134:1227-1233.
- Akiskal HS. A developmental perspective on recurrent mood disorders: a review of studies in man. Psychopharmacol Bull 1986;22;579-586.
- Rosenthal TL, Akiskal HS, Scott-Strauss A, Rosenthal PH David M. Familial and developmental factors in characterological depressions, J Affect Disord 1981;3:183-192.
- Klein DN, Taylor EB, Harding K. Double depression and episodic ma- jor depression: demographic, clinical, familial, personality, and socio-
- environmental characteristics and short term out come. Am J Psychiatry 1998;145:1226-1231.
- Rhimer Z. Dysthymia: a clinicians' perspective. In: Burton S, Akiskal HS, editors. Dysthymic disorder. London: Royal College of Psychiatrists; 1990:112-125.
- Kovacs M, Akiskal HS, Gatsonis C, Farrow PL. Childhood-onset dys- thymic disorder: clinical features and prospective naturalistic outcome. Arch Gen Psychiatry 1994;51:365-374.
- Von Zerrsen D, Possl J. The premorbid personality of patients with different subtypes of an affective illness. Statistical analysis of blind assignment of case history data to clinical diagnosis. J Affect Disord 1990;18:39-50.
- Akiskal HS. Developmental pathways to bipolarity: are juvenile onset depressions pre-bipolar? J Am Acad Chid Adol Psychiatry 1995;34: 754-763.
- Hantouche EG, Akiskal HS, Lancrenon S, et al. Systematic clinical methodology for validating bipoolar-II disorder: data in midstream from a French national multisite study (EPIDEP). J Affect Disord 1998;50: 163-173.
- Depue RA, Slater JF, Wolfstetter-Kausch H, et al. A behavioral para- digm for identifying persons at risk for bipolar depressive disorder: a conceptual framework and five validating studies. J Abnorm Psychol 1981;90:381-437.
- Cassano GB, Akiskal HS, Savino M, Musetti L, Perugi G, Soriani A. Proposed subtypes of bipolar II disorder: with hypomanic episodes and/ or with hyperthymic temperament. J Affect Disord 1992;26:127-140.
- Akiskal HS, Hantouche EG, Bourgeois M, et al. Gender, temperament and the clinical picture in dysphoric mixed mania: findings from a French national study (EPIMAN). J Affect Disord 1998;50:175-186. Perugi G, Maremmani I, Toni C, Madaro D, Mata B, Akiskal HS. The contrasting influence of depressive and hyperthymic temperaments on psychometrically derived manic subtypes. Psychiatry Res 2001;101: 249-258.
- Henry C, Lacoste J, Bellivier F, Verdoux H, Bourgeoise ML, Leboyer M. Temperament in bipolar illness: impact on prognosis. J Affect Disord 1999;56;103-108.
- Perugi G, Akiskal HS., Micheli C, et al. clinical subtypes of bipolar mixed states : validating a broader European definition in 143 cases. J Affect Disord 1997;43:169-180.
- Akiskal HS. the distinctive mixed states of bipolar I, II, and III. Clin. Neuropharmacol 1992;15:632-633.
- Cassano GB, Akiskal HS, Perugi G, Musetti L, Soriani A, Mignani V. Psychopathology, temperament, and past course in primary major Mundt CH, editor. Interpersonal factors in the origin and course of depressions. Psychopathology 1989;22:278-288.
- Cassano GB, Akiskal HS, Perugi G, Musetti L, Savino M. The importance of measures of affective temperaments in genetic studies of mood disorders. J Psychiatr Res 1992;26:257-268.
- Montgomery SA, Asberg M. A new depressed scale designed to be sensitive to change. Br J Psychiatry 1979;134:382-389.
- Refaelsen BP, Bowling OJ, Kramp TG. The Bech-Refaelsen Mania Rating Scale and Hamilton Depression Rating Scale. Acta Psychiatr Scand 1979;59:420-430.
- Akiskal HS, Mallya G. Criteria for the 'soft' bipolar spectrum. Treat- ment implications. Psychopharmacol Bull 1987;23:68-73.
- Placidi GF, Signoretta S, Liguori A, Gervasi R, Maremmani I, Akiskal HS. The semi-structured affective temperament interview (TEMPS-1): reliability and psychometric properties in 1010 14-26 year old students. J Affect Disord 1998;47:1-10.
- Eysenck HJ, Eysenck SBG. Manual of the Eysenck Personality Questionnaire. London: Holder and Stoughton; 1975.
- Cloninger CR. A systematic method for clinical description and classi- fication of personality variants. A proposal. Arch Gen Psychiatry 1987; 50;573-588.
- Goldman HH, Skodol AE, Lave TR. Revising axis V for DSM IV: A review of measures of social functioning. Am J Psychiatry 1992;149: 1148-1156.
- Klein DN. Depressive personality: reliability, validity, and relation to dysthymia. J Abnorm Psychol 1990;99:412-421.
- Akiskal HS. Dysthymia, cyclothyrnia and related chronic subthresh- old mood disorders. In: Gelder M, Lopez-lbor J, Andreasen N, editors. New Oxford textbook of psychiatry. Oxford: Oxford University Press; 2000:736-749.
- Akiskal HS. Mood disorders: clinical features. In: Sadock BJ, Sadock VA, editors. Comprehensive textbook of psychiatry. Vol, 1. 7th ed. Baltimore: Williams and Wilkins; 2000:1169-1198.
- Akiskal HS, Akiskal K. Cyclothymic, hyperthymic and depressive tem- peraments as sub affective variants of mood disorders. In: Tasman A, Riba MB, editors. American Psychiatric Association review. Washington: American Psychiatric Press; 1992:43-62.
- Angst J. The course of affective disorders. II. Typology of bipolar manic depressive illness. Arch Psychiatr Nervenkr 1978;226:65-73.
- Quitkin FM, Rabkin JG, Prien RF. Bipolar disorders: are there manic- prone and depressive- prone forms? J Clin Psychopharmacol 1986;6: 167-172.
- Coryell W, Turvey C, Endicott J, et al. Bipolar I affective disorder: predictor of outcome after 15 years. J Affect Disord 1998;50:109-116. 39. Musetti L, Perugi G, Soriani A, Rossi VM, Cassano GB, Akiskal HS.
- Depression before and after age 65: a re-examination. Br J Psychiatry 1989;155:330-336.
- Perugi G, Musetti L, Simonini E, Piagentini F, Cassano GB, Akiskal Affective Temperaments and Polarity in Bipolar Disorder
- Gender mediated clinical features of depressive illness: the impor- tance of temperamental differences. Br J Psychiatry 1990;157:835-847. Niculescu AB III, Akiskal HS. Proposed endophenotypes of psychiatry: evolutionary, clinical, and pharmacogenomic considerations. Mol Psy- chiatry 2001;6:363-366.
- Akiskal HS. Characterological manifestations of affective disorders. Towards a new conceptualization. Integer Psychiatry 1984;2:83-88.
- Eckbald M, Chapman LJ. Development of a scale of hypomanic personality. J Abnorm Psychol 1986;95:214-222.
- Cloninger CR, Bayon C, Svrakic DM. Measurement of temperament and character in mood disorders: a model of fundamental states as per- sonality types. J Affect Disord 1998;51:21-32.
- Angst J, Clayton P. Premorbid personality of depressive, bipolar and schizophrenic patients with special reference to suicidal issues. Compr Psychiatry 1986;27:511-532.
- Clark DC. Narcissistic cries of aging and suicidal despair. Suicide Life Threatening Behav 1993;23:21-26.
- Martin RL, Cloninger CR, Guze SB, Clayton PJ. Mortality in a follow- up of 500 psychiatric out-patients. II. Cause-specific mortality. Arch Gen Psychiatry 1985;42:58-66.
- Angst A, Sellaro R. Historical perspectives and natural history of bipo- lar disorder. Biol Psychiatry 2000;48:445-457.
