
Hong Kong J Psychiatry 2008;18:15-22
ORIGINAL ARTICLE
A Survey on Same-sex Attraction in Secondary School Adolescents: Prevalence and Psychosocial Factors
一項關於中學生同性吸引的問卷調查:流行率和心理社會因素
KK Wu, EY Leung, AY Leung
胡潔瑩、梁若芊、梁艷枝
KK Wu, PhD, M. Soc. Sc (Clin. Psy.), Department of Psychology, The Chinese
University of Hong Kong, Shatin, Hong Kong, China.
EY Leung, PhD, M. Soc. Sc. (Clin. Psy.), Centre of Development and Resources for Students, The University of Hong Kong, Hong Kong, China.
AY Leung, BSW, Miracle Loops Consulting Services Limited, Hong Kong, China.
Tel: (852) 3408 7439; Fax: (852) 2307 5894; E-mail: wukyk@ha.org.hk
Submitted: 19 July 2007; Accepted: 24 September 2007
Abstract
Objective: To investigate subjective certainty regarding same-sex attraction and related psychosocial factors in youths.
Participants and Methods:Questionnaire survey of 413 secondary school students (aged 12 to 21 years).
Results: In all, 21% of the participants reported uncertainty about same-sex attraction and 4% reported definitely being same-sex attracted. Females were more likely than males to report uncertainty or certainty about same-sex attraction, and a higher level of perceived knowledge by peers on their sexual orientation. Males were more likely than females to report being not same-sex attracted. The level of satisfaction with one's gender identity was not significantly low for those who were certainly same-sex attracted, but participants who were unsure of same-sex attraction were less satisfied with their gender identity than those who were definitely not same-sex attracted. Participants who were same-sex attracted or unsure of same-sex attraction had lower perceived levels of acceptance and experienced more victimisation about their sexual orientation within their social environment, than those who reported they were not same-sex attracted.
Conclusion:It is important not to have a preconception about the sexual orientation of individual youths in healthcare settings. Same-sex attraction is associated with subjective feelings of an unfavourable social environment.
Key words: Bisexuality; Crime vicims; Gender identity; Homosexuality; Mental health
摘要
目的:研究有關青少年同性吸引的主觀肯定程度和相關心理社會因素。
參與者與方法:413名12至21 歲的中學生接受問卷調查。
結果:調查結果顯示:,21%中學生不肯定是否受同性吸引,4%則肯定受同性吸引。相對男生,較多女生表示不肯定或肯定自己受同性吸引和認為朋輩知道自己的性取向;相對女生,較多男生表示肯定不受同性吸引。肯定自己受同性吸引的,對己身性別的滿意水平並不特別低;而對不肯定是否受同性吸引的,他們對己身性別的滿意度則不及那些肯定不受同性吸引的。不論肯定或不肯定是否受同性吸引的,相對於肯定不受同性吸引的,他們皆認為外間對己身的性取向接受的程度偏低,亦因己身的性取向在社交上有較多被傷害的經驗。
結論:在提供醫療服務時不應對青少年的性取向作出假設的判斷。同性吸引與主觀不利的社交 環境是有關聯的。
關鍵詞:兩性體、受害者、性別身份、同性戀、精神健康
Introduction
Studies on sexual orientation, especially on youths, are under- represented in the clinical and research literature. Studies in the West have provided some information for discussion of the issue. However, there is still inadequate research in this area, especially in Asian countries. According to McGough,1 an anthropologist who studied deviant marriage patterns in Chinese societies, same sex unions for women and men, and institutionalised relationships between males in some areas of China have been documented in traditional Chinese societies. However, there were not enough data to reveal how common these ‘deviant’ forms of marriage were. Though non-heterosexuality, including lesbian, gay, bisexual and transgender (LGBT) youths do exist in the modern Chinese society of Hong Kong, and some do present to child and adolescent clinical services, there is a lack of well-documented studies on the prevalence of different sexual orientations and social distress among this population. Yet, research in western countries has shown that more and more young people are ‘coming-out’ while still of school age.2 Other studies have also shown that non-heterosexual youths were significantly more likely to engage in health risk behaviours than their peers. These behaviours included substance use, violent assault, unsafe sexual practices, and suicidal behaviour.3-5 Other threats to health among adult gay men and lesbians have also been the subject of increasing attention.6
According to D’Augelli,7 the lack of affirmation experienced by young people as they begin to construct their non-heterosexual identities can have significant effects on their development. Moreover, as non-heterosexual youths often spent their formative years hiding their sexual orientation from others, little is known about their normative developmental patterns. Thus, it is not clear if being non- heterosexual causes a young person to engage in health risk behaviours, or if other factors, such as social stigmatisation and victimisation, lie at their root. Past research suggested that experiences of intolerance play a part in alienating non-heterosexual youths.7,8 Non-heterosexual youths were found to have experienced rejection and discrimination within the family and school, presumably because of their sexual orientation.9,10 Victimisation has also been related to social hostility towards homosexuality.11 The nature of the victimisation experience might vary between cultures. British gay and bisexual men were found to experience more physical, verbal, sexual victimisation and property damage than their American counterparts. However, rates of victimisation were substantially higher in secondary, junior high and high schools in America than in Britain.12
Investigation of the development of homosexuality has tended to focus on adults with an established homosexual identity reporting their earlier experiences. This tells us little about those who have transient same-sex attraction and experience at younger ages. Longitudinal studies have mainly followed groups recruited through gay, bisexual, lesbian and women’s studies networks, rather than the general population.13,14 A longitudinal study in the general population conducted on a New Zealand cohort of about 1,000 people, analysed their self-reported same-sex attraction at age 21 and 26 years, and found that occasional same-sex attraction was common. By age 26, 10.7% of men and 24.5% of women reported being attracted to their own sex some time. Between age 21 and 26, there were more men who moved away from an exclusively heterosexual attraction (1.9%) than moved towards it (1.0%), while for women, many more moved away (9.5%) than towards an exclusive heterosexual attraction. This indicated that same- sex attraction was not exclusive and was unstable in early adulthood, especially among women.15 The results of this study conducted in the general population were consistent with findings of a study on sexual-minority young American women over a 2-year period, which found that half of the participants had changed orientations more than once within the period of study.16 Based on major findings of their series of research programmes on female sexuality, Diamond and Savin-Williams17 suggested that the timing of a woman’s first same-sex attraction does not predict their stability of sexual identity, and the variability in sexual-minority and heterosexual women’s sexual development is best explained by interaction between personal characteristics and the environment.
Studies of adults with gender identity disorder, especially those who are sexually attracted to members of their own biological sex, show early childhood onset of cross-gender behaviour and the wish to be the opposite sex.18,19 However, studies of children referred clinically for gender identity issues found that the majority developed homosexual orientation with no desire for sex change, and only a minority persist with the desire to change their sex upon reaching adolescence or young adulthood.20,21 Thus, the relationship between gender identity disorder and non-heterosexual sexual orientation appear to be related, but independent of each other, when viewed from a developmental prospective.
In Hong Kong, local studies have been conducted to examine sex roles, attitudes, and behaviour of youths.22,23 According to a local survey examining attitudes of adolescents towards homosexuality, only 21.5% of respondents indicated that homosexuals were accepted and 70.8% indicated that homosexuals were not accepted by the Hong Kong society.24 When the present study was conducted, the authors were not aware of any other study on different sexual orientations and related gender identity issues, based on self-reporting among youths in Hong Kong or in any other Chinese society.
Given the very limited data on sexual orientation among Chinese youths, the present study aimed to examine the occurrence of same-sex attraction among youths in Hong Kong (a modern westernised city in China). The effect of gender and sexual orientation on acceptance of one’s sexual orientation, gender identity, knowledge and perceived reaction from others to one’s sexual orientation, and experience of victimisation were examined. It was expected that there were more similarities than differences in the developmental process of sexual identity and orientation between youths in Hong Kong and in the West. While the majority of youths were likely to affirm being definitely not same-sex attracted, some were expected to experience uncertainty, and a minority were expected to affirm being same-sex attracted. Based on western findings, it was hypothesised that females are more likely than males to report uncertainty or inclination for same-sex attraction. Since same-sex sexuality violates current culturally defined sexual norms in Hong Kong, it was hypothesised that youths reporting undecided or affirmed same-sex attraction would experience rejection in their family and school, due to their minority sexual orientation. The effect of gender on sexual orientation and associated psychosocial experience was therefore examined in the context of differing social status and roles assigned for males and females in Chinese societies.
Methods
Participants
Students from five secondary schools in different districts served by The Boys’ and Girls’ Clubs Association (BGCA), one of the largest non-government organisations providing community social and recreation services for youths in Hong Kong, were selected. They participated in this study anonymously during the academic year of 2002 to 2003. Forms 1 to 7 students taken from 1-2 classes (13 classes altogether) from these schools were invited to participate in the study. The survey was approved by the Guidance Committee in these schools and School Social Work Unit of BGCA.
With parental consent, 413 secondary school students aged 12 to 21 years participated in the study; their mean age was 15.6 (SD, 2.1) years. Among them, 174 (42.1%) were males, 237 (57.4%) were females, and 2 (0.4%) did not report their gender. Eighty three (20.1%) were studying in boy schools, 173 (41.9%) in girl schools, and 157 (38.0%) in co-educational schools. The questionnaires were administered in their respective schools; the return rate of the questionnaire was 100%, and the rate of full completion was 98.7%.
Procedure and Measures
A self-administered questionnaire written in Chinese was administered in the classroom. To ensure confidentiality, the classroom was arranged as if for an academic examination. Thus, each participant occupied a single table with a few feet between them so that they could not read each other’s responses. Measures ensuring confidentiality of data were explained before the questionnaires were distributed. Such measures included: anonymous return, identification only by code numbers, and an envelope for the questionnaire provided for each participant. Upon completion, each questionnaire was returned directly to the research assistants in a sealed envelope.
The self-administered questionnaire was designed by an expert focus group based on literature review of related studies.8,12 The focus group comprised a clinical psychologist and a group of school social workers working in secondary schools. The items generated were consolidated and the questionnaire was given to a group of secondary school students at the target age range for their comments and feedback on feasibility. The final questionnaire was completed after minor alterations to the phrasing.
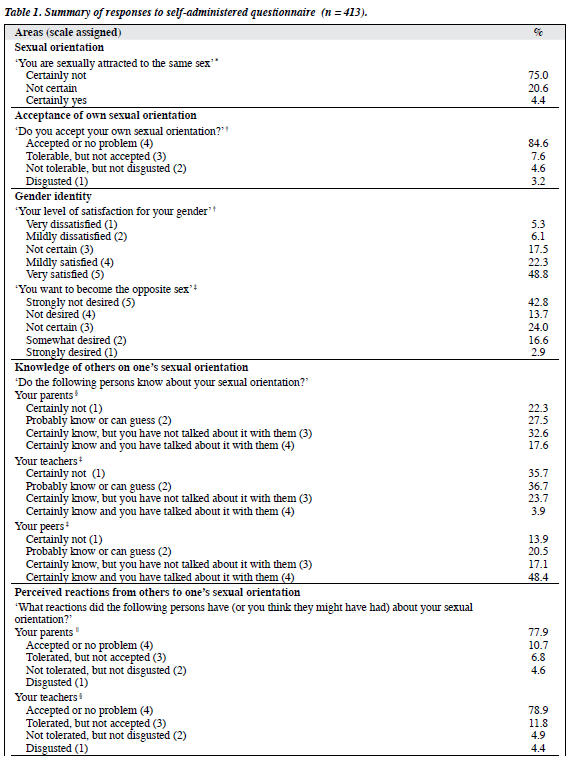
The questionnaire assessed the following areas: (1) certainty of same-sex attraction, (2) acceptance of one’s own sexual orientation, (3) gender identity, (4) perceived level of knowledge of others on one’s sexual orientation, (5) perceived reactions from others to one’s sexual orientation, (6) frequency of experiencing victimisation in terms of being reprimanded or alienated by others due to one’s sexual orientation.
The certainty of same-sex attraction among participants was studied by examining participants’ responses to the statement ‘You are sexually attracted to the same sex’. Their choice of response differentiated the participants into 3 categories: certainly same-sex attracted, unsure of same-sex attraction, and certainly not same-sex attracted.
Participants’ responses to the statement ‘Do you accept your own sexual orientation?’ were ranked on a 4- point scale with 1 (disgusted) indicating the lowest level of acceptance, to 4 (accepted or no problem) indicating the highest level of acceptance.
Participants’ responses to the statement ‘Your level of satisfaction for your gender’ were ranked on a 5-point scale with 1 (very dissatisfied) indicating the lowest level of satisfaction, to 5 (very satisfied) indicating the highest level of satisfaction.
Participants’ responses to the statement ‘You want to become the opposite sex’ were ranked on a 5-point scale with 1 (strongly desired) to 5 (strongly not desired).
Participants’ responses to the statement ‘Do the following persons know about your sexual orientation?’ were ranked on a 4-point scale with 1 (certainly not) indicating the lowest level of knowledge to 4 (certainly and you have talked about it with them) indicating the highest level of knowledge by parents, teachers, and peers, respectively.
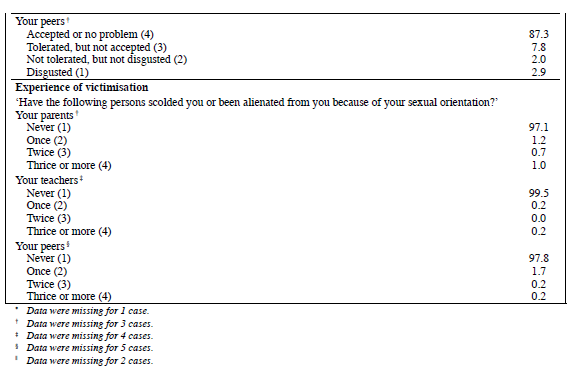
To examine the participants’ perceived reactions of their parents, teachers and peers towards their sexual orientation, responses to the statement ‘What reactions did the following persons have (or you think they might have had) about your sexual orientation?’ were ranked on a 4- point scale with 1 (disgusted) indicating the lowest level of acceptance to 4 (accepted or no problem) indicating the highest level of acceptance.
To examine participants’ experience of victimisation (i.e. being reprimanded or alienated by others) due to their sexual orientation, responses to the following statement ‘Have the following persons scolded or been alienated from you because of your sexual orientation?’ were ranked on a 4-point scale, scoring 1 (never) indicating the lowest level of victimisation, to 4 (thrice or more) indicating the highest level of victimisation coming from parents, teachers, and peers. The content and Likert scale assigned for each item and descriptive results of the survey are shown in Table 1.
Results
Sexual Orientation, Gender and Age
In all, 410 (99.3%) of the participants replied to the statement on certainty of same-sex attraction. Chi-square tests revealed that there were significantly more females (29.1%) than males (9.2%) who were unsure about same- sex attraction, and more females (5.9%) than males (2.3%) who were definitely same-sex attracted (χ2 [2] = 29.33, p < 0.001, effect size (ES) = 0.26).
Results of two-way analysis of variance (ANOVA) indicated that the main and interaction effects of gender and sexual orientation on age were not significant (p > 0.05).
Gender, Sexual Orientation and Psychosocial Variables
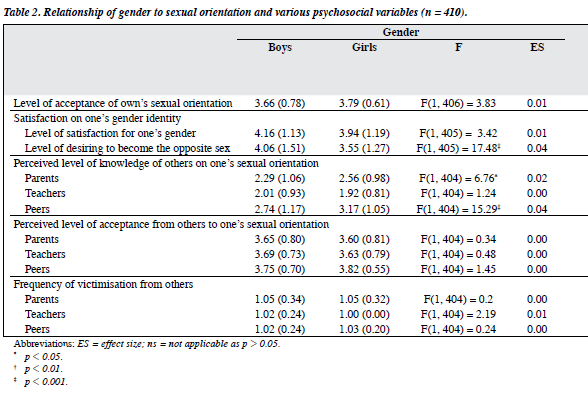
Since the number of males who were definitely same- sex attracted was too few for examination of interaction effects between gender and sexual orientation, only the independent effects of gender and sexual orientation on various psychosocial factors were examined. To examine independent effects on the level of acceptance of one’s own sexual orientation, ANOVA was used. For other psychosocial variables defined by more than 1 item, the independent effects of gender and sexual orientation were studied by multivariate analysis of variance (MANOVA) followed by univariate F tests for individual variables.
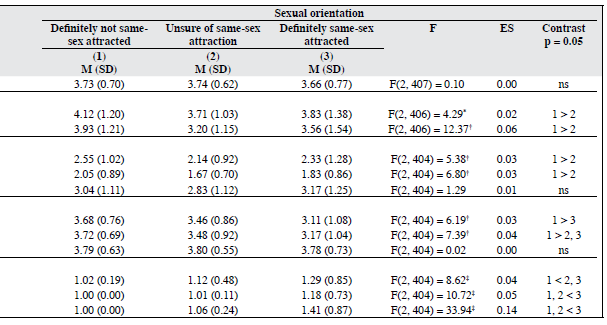
The effect of gender was significant for the combined dependent variables for satisfaction on one’s gender identity; Pillai’s = 0.04, F(2, 404) = 9.04, p < 0.001, ES = 0.04, and perceived level of knowledge of others for one’s sexual orientation, Pillai’s = 0.08, F(3, 402) = 11.61, p < 0.001, ES = 0.08. The effect of sexual orientation was significant for combined dependent variables pertaining to satisfaction with one’s gender identity; Pillai’s = 0.07, F(4, 812) = 6.77, p < 0.001, ES = 0.03; perceived level of knowledge of others for one’s sexual orientation, Pillai’s = 0.04, F(6, 806) = 2.83, p = 0.01, ES = 0.02; perceived reactions from others to one’s sexual orientation, Pillai’s = 0.08, F(6, 806) = 5.40, p < 0.001, ES = 0.04, and frequency of experiencing victimisation, Pillai’s = 0.16, F(6, 806) = 11.72, p < 0.001, ES = 0.08. As shown in Table 2, the significant impact of gender and sexual orientation on a particular combined dependent variable described above was also significant according to univariate F tests for most individual variables addressed with the respective combined dependent factors (Table 2).
Discussion
Consistent with the findings of a longitudinal study on the general adult population in New Zealand,15 uncertainty about one’s sexual orientation was expressed by 21% of the participants. It reveals that sexual orientation could be undecided for youths. Sexual orientation for many young persons is not exclusively heterosexual or homosexual. In the present study, females were more likely to admit uncertainty about their sexual orientation, which is consistent with the findings reported by Dickson et al.15 Results of this study also provide preliminary support for the potential application of the conceptual approach to the study of female same-sex sexuality for Asian youths, which aims to explain the diverse developmental trajectories observed by American researchers.17 Based on a series of research projects on sexual-minority females, they proposed that women’s attraction could be non-exclusive and fluid. They also suggested that there was considerable variation in the quality and distribution of women’s same-sex and other-sex attractions, as well as the context in which these were experienced. Moreover, they proposed that variability in sexual-minority and heterosexual women’s sexual development is best explained by interactions between personal characteristics and the environment.
The present findings have meaningful clinical implications. It is important not to have preconceptions about the sexual orientation of individual adolescents. Assumption of heterosexuality might be perceived as a disregard of the uncertain sexual orientation experienced by one-quarter of young people. As suggested in a recent review, assuming that the youths we work with are heterosexual may inadvertently give a message about how open we are with respect to sexual-minority individuals, who have not fully accepted their sexual orientation. Such a message may appear to confirm that they are not normal.25
The present study found that the level of acceptance of one’s sexual orientation among youths is unrelated to sexual orientation. Though young persons who are distressed by their sexual orientation may be less likely to report their divergent sexual orientation in a survey of this kind, a significant percentage nevertheless revealed their uncertainty. Moreover, the level of acceptance of their sexual orientation that they reported was not different from those claiming to be not same-sex attracted with certainty. This implies that sexual-minority orientation does not necessarily lead to ego-dystonic type of distress. Results of the present study are inconsistent with the position of some researchers, who argue that same-sex attraction is pathological. According to their view it is justifiable to offer psychological treatment for such youths, with the aim of converting them from being homosexuals (or unsure about same-sex attraction) into becoming heterosexuals.26 In the present study, some participants reported being certainly same-sex attracted, whilst uncertainty about same-sex attraction was not uncommon, and yet these youths were not distressed by their own sexual-minority orientation. This contradicts the belief that young persons who are homosexuals or unsure of same-sex attraction are prone to persistent and marked distress and require various forms of treatment to reduce stress. Results of the present study suggest that clinicians should avoid labelling the uncertainty experienced in adolescence as a mental disorder.
Based on findings in the West it is also important to recognise that the lack of affirmation experienced by sexual- minority youths, as they begin to construct their sexual identities can have a negative impact on their development.7 The level of satisfaction with one’s gender identity is not particularly low for those who reported themselves as same- sex attracted. This supports the notion that homosexual orientation and gender identity disorder are independent from each other. Nevertheless, young persons who are unsure of same-sex attraction are less satisfied with their gender identity than those who are definitely not same-sex attracted and may experience hesitation and ambivalence towards their gender identity.
Though same-sex attraction does not affect self- acceptance, the present study reveals that such youths perceive their parents and teachers to have a lower level of acceptance for their sexual orientation and experience more victimisation from parents, teachers and peers than not same-sex attracted persons. Youths who are unsure of same-sex attraction also share the social distress faced by youths who are definitely same-sex attracted, as they have lower perceived levels of acceptance from their teachers and more of them experience victimisation from parents, compared to those who are definitely not same-sex attracted. The likely unfavourable family and social environment subjectively faced by sexual-minority youths in Hong Kong is consistent with findings in the West, where youths with undecided or same-sex sexual orientation are vulnerable to rejection and discrimination.9-11 In addition, previous research has found that sexual-minority stress experienced by youths differs from stress experienced by most racial and religious minorities, because family can be a powerful support in coping for the latter groups. However, parents’ initial reactions to sexual-minority adolescents ‘coming out’ usually involve negative emotions and rejections.9,27 Sexual-minority youths are also harassed at school,10 where they appear to receive limited social support, are liable to experience rejection and / or may be alienated by peers, parents and teachers. Healthcare professionals working with youths therefore need to be sensitive to the needs and stresses for sexual-minority young persons. Acknowledging the existence of sexual-minority and uncertainty about sexual orientation in youths is a first step. Other measures include encouraging the development of a supportive environment through education, and the provision of early supportive services for youths distressed by the psychosocial impact of rejection and discrimination.
The present study was limited by having to rely on convenience sampling and the questionnaire that was adopted. The reliability and validity of the questionnaire have not been examined in order to reduce the risk of identity disclosure. Thus, the present study should be considered as a survey collecting self-reported responses from a group of youths. It was not a means of categorising young people into different sexual orientations based on a reliable and locally validated screening / diagnostic tools. The validity of items measuring frequency of social victimisation is limited by participants’ self-reporting responses; thus, the social reactions and victimisation documented are based on subjective interpretation of life experiences. To delineate the level of certainty about same-sex attraction, participants were asked to choose between ‘certainly not’, ‘not certain’, and ‘certainly yes’. It is possible that the choices of ‘certainly not’ and ‘certainly yes’ were so strong that they affected the responses by increasing the tendency of participants to choose ‘not certain’ as their answer. If this confounding effect really exists, it is possible that responses may have differed if the choices were simply: ‘yes’, ‘not certain’, and ‘no’. Since it is a sensitive and difficult matter to express uncertainty for same-sex attraction and the low likelihood for youths to report divergent sexual orientation, the strong and distinctive alternatives used probably facilitated the expression of any uncertainty. However, the present choice of ‘certainly yes’ may have made it more difficult for participants to affirm themselves as same-sex attracted. Though confidentiality is assured, the likelihood of under- reporting may still exist as the validity of administering a questionnaire on sexual issues in a Chinese classroom context is not certain and participants might not be convinced of confidentiality, while the stigma of exposing one’s non- heterosexual orientation could be paramount.
This study was also limited by the small sample size of participants who were certain about same-sex attraction, whilst a much larger group indicated their uncertainty. Thus, the results may be more able to reflect the situation of youths who were uncertain than the situation faced by LGBT youths, who felt certain about their sexual orientation.
The present study was not longitudinal, which is important if one wants to reach conclusions about the fluidity of sexual orientation. Longitudinal study of the development of sexual orientation for youths, particularly those expressing uncertainty about their sexual orientation, could facilitate understanding of the corresponding developmental trajectory in young persons. Further studies on the relationship between psychosocial distress and mental health of youths attracted to the same sex, and how such orientation relates to traditional Chinese and western beliefs are suggested.
Acknowledgements
The study was supported by The Boys’ and Girls’ Clubs Association of Hong Kong. We would like to thank Eva Ho for her assistance in the planning of the study, data collection and analysis, and Mabel Tse for her clerical assistance.
References
- McGough JP. Deviant marriage patterns in Chinese society. In: Kleinman A, Lin T, editors. Normal and abnormal behavior in Chinese culture. Dordrecht, Holland: D. Reidel Publishing Co.; 1981: 171-201.
- Pilkington NW, D’Augelli AR. Victimization of lesbian, gay, and bisexual youth in community settings. J Community Psychol 1995;23:33-56.
- Rosario M, Hunter J, Gwadz M. Exploration of substance use among lesbian, gay and bisexual youth: prevalence and correlates. J Adolesc Res 1997;12:454-76.
- Rotheram-Borus M, Rosario M, Van Rossem R, Reid H, Gillis R. Prevalence, course, and predictors of multiple problem behaviors among gay and bisexual male adolescents. Dev Psychol 1995;31:75- 85.
- Fergusson DM, Horwood LJ, Beautrais AL. Is sexual orientation related to mental health problems and suicidality in young people? Arch Gen Psychiatry 1999;56:876-80.
- Northridge ME. Advancing lesbian, gay, bisexual and transgender health [Editorial]. Am J Public Health 2001;91:855-6.
- D’Augelli AR. Identity development and sexual orientation: Towards a model of lesbian, gay, and bisexual development. In: Trickett EJ, Watts RJ, Birman D, editors. Human diversity: perspective on people in context. San Francisco: Jossey-Bass; 1994: 118-32.
- D’Augelli AR. Mental health problems among lesbian, gay, and bisexual youths ages 14 to 21. Clin Child Psychol Psychiatry 2002;7:433-56.
- Boxer AM, Cook JA, Herdr G. Double jeopardy: identity transitions and parent-child relations among gay and lesbian youth. In: Pillemer K, McCartney K, editors. Parent-child relations throughout life. Hillsdale, NJ: Erlbaum; 1991: 59-92.
- Mental Health America. “What does gay mean?” Study, 2002. Website: http://www.mentalhealthamerica.net/go/whatdoesgaymean/ whatdoesgaymean. Accessed 18 January 2008.
- Russell ST, Franz BT, Driscoll AK. Same-sex romantic attraction and experience of violence in adolescence. Am J Public Health 2001;91:903-6.
- Carragher DJ, Rivers I. Trying to hide: a cross-national study of growing up for non-identified gay and bisexual male youth. Clin Child Psychol Psychiatry 2002;7:457-74.
- Diamond LM. Development of sexual orientation among adolescent and young adult women. Dev Psychol 1998;34:1085-95.
- Pattatucci AM, Hamer DH. Development and familiarity of sexual orientation in females. Behav Genet 1995;25:407-20.
- Dickson N, Paul C, Herbison P. Same-sex attraction in a birth cohort: prevalence and persistence in early adulthood. Soc Sci Med 2003;56:1607-15.
- Diamond LM. Sexual identity, attractions, and behavior among young sexual-minority women over a 2-year period. Dev Psychol 2000;36:241-50.
- Diamond LM, Savin-Williams RC. Explaining diversity in the development of same-sex sexuality among young women. Psychological perspectives on lesbian, gay, and bisexual experiences. 2nd ed. New York: Columbia University Press; 2003: 130-48.
- Blanchard R. Nonhomosexual gender dysphoria. J Sex Res 1988;24:188-93.
- Freund K, Langevin R, Satterberg J, Steiner B. Extension of the Gender Identity Scale for males. Arch Sex Behav 1977;6:507-19.
- Cohen-Kettenis PT. Gender identity disorder in DSM? [Letter]. J Am Acad Child Adolesc Psychiatry 2001;40:391.
- Green R. The ‘sissy boy syndrome’ and the development of homosexuality. New Haven, CT: Yale University Press; 1987.
- Research of sex role, attitude and behaviour of youth in Hong Kong. Hong Kong: Breakthrough; 1994.
- The Family Planning Association. Youth sexuality study 2001: In- school youth, Hong Kong: The Family Planning Association of Hong Kong; 2002.
- Hong Kong Federation of Youth Groups. Survey on acceptance level of youths in Tsuen Wan for homosexuality. Hong Kong: Hong Kong Federation of Youth Groups; 1999.
- Eubanks-Carter C, Burckell LA, Goldfried MR. Enhancing therapeutic effectiveness with lesbian, gay, and bisexual clients. Clin Psychol Sci Pract 2005;12:1-18.
- Nicolosi J, Nicolosi LA. A parent’s guide to preventing homosexuality. Downers Gove, IL: InterVarsity Press; 2002.
- Robinson BE, Walters LH, Skeen P. Response of parents to learning that their child is homosexual and concern over AIDS: A national study. J Homosex 1989;18:59-80.
