
East Asian Arch Psychiatry 2012;22:110-3
THEME PAPER
日本一所为早期思觉失调患者而设的多维治疗中心的临床实践
A/Prof. Takahiro Nemoto, MD, PhD, Department of Neuropsychiatry, Toho University School of Medicine, Japan.
Dr Tomoyuki Funatogawa, MD, Department of Neuropsychiatry, Toho University School of Medicine, Japan
Dr Miki Tobe, MD, Department of Neuropsychiatry, Toho University School of Medicine, Japan.
Dr Taiju Yamaguchi, MD, PhD, Department of Neuropsychiatry, Toho University School of Medicine, Japan.
Dr Keiko Morita, MD, Department of Neuropsychiatry, Toho University School of Medicine, Japan.
Dr Naoyuki Katagiri, MD, PhD, Department of Neuropsychiatry, Toho University School of Medicine, Japan.
Dr Naohisa Tsujino, MD, PhD, Department of Neuropsychiatry, Toho University School of Medicine, Japan.
Prof. Masafumi Mizuno, MD, PhD, Department of Neuropsychiatry, Toho University School of Medicine, Japan.
Address for correspondence:A/Prof. Takahiro Nemoto, Department of Neuropsychiatry, Toho University School of Medicine, 6-11-1 Omori-Nishi, Ota-ku, Tokyo 143-8541, Japan.
Tel: (81-3) 3762 4151; Fax (81-3) 5471 5774; email: takahiro.nemoto@med.toho-u.ac.jp
Submitted: 13 April 2012; Accepted: 1 July 2012
Abstract
Early intervention for psychosis in Japan has lagged behind that in western countries, but has rapidly begun to attract attention in recent years. As part of a worldwide trend, a multi-dimensional treatment centre for early psychosis consisting of a Youth Clinic, which specialises in young individuals with an at-risk mental state for psychosis, and Il Bosco, a special day-care service for individuals with early psychosis, was initiated at the Toho University Omori Medical Center in Japan in 2007. The treatment centre aims to provide early intervention to prevent the development of full-blown psychosis in patients with an at-risk mental state and intensive rehabilitation to enable first-episode schizophrenia patients to return to the community. We presently provide the same programmes for both groups at Il Bosco. However, different approaches may need to be considered for patients with an at-risk mental state and for those with first- episode schizophrenia. More phase-specific and need-specific services will be indispensable for early psychiatric interventions in the future.
Key words: Cognitive therapy; Early intervention (education); Japan; Schizophrenia
摘要
虽然日本的思觉失调早期干预服务落後於西方国家,但近年开始备受注意。思觉失调早期干预 已成全球趋势,有见及此,日本东邦大学大森病院於2007年成立针对思觉失调的多维治疗中 心,包括为思觉失调潜伏期年青人提供服务的「青年诊所」,和以早期思觉失调患者为对象的 日间精神复康中心「Il Bosco」,旨在为潜伏期患者提供早期干预以抑制典型思觉失调病发,以 及为首发精神分裂症患者提供密集式复康服务,使他们能尽快重投社会。虽然Il Bosco正实施上 述两种治疗计划,不过也须考虑这两类患者的需要而采用合适的治疗方案。阶段性和患者为本 服务是思觉失调早期干预计划发展必不可少的部份。
关键词:认知治疗、早期干预(教育)、日本、精神分裂症
Early Psychiatric Intervention in Japan
Early intervention for psychosis in Japan has lagged behind that in western countries because of the continued existence of hospital-based psychiatry which requires large numbers of psychiatric beds and long-term hospital stays,1 as well as barriers resulting in delayed patient contact with psychiatric services. However, early intervention has rapidly begun to attract attention in recent years.2 Despite the difficult circumstances, reports indicated that earlier detection may enable better outcomes in addition to shortening the duration of untreated psychosis (DUP) in Japan.3,4 The energetic activities of the Japanese Society for Prevention and Early Intervention in Psychiatry (Website: http://www.jseip.jp) have also promoted early psychiatric interventions. The latest multicentre retrospective study in Japan revealed that the mean and median DUP were 20.3 and 6.0 months, respectively.5
When thinking about the dissemination of early intervention for mental disorders in Japan, we must consider the culture and attitudes towards mental disorders among the Japanese people. In the light of our own clinical experience, individuals with mental health problems and their families are often reluctant to seek help for various reasons, including ignorance about the features and treatability of mental disorders, beliefs that the problem should be solved by themselves, confining the problem to close relations without consulting professionals, and stigma connected with psychiatry, although Japanese people generally accept the need for medical treatment for physical problems. These obstacles may explain the long DUP and the social stigma towards mental disorders in Japan. However, the nuclearisation of families may also be affecting this delay in seeking treatment. Nishii et al5 reported that patients living alone in Japan had significantly longer DUP than those living with their families. These considerations should be further investigated.
Some treatment services specialising in the early stage of psychosis have recently been established in Japan, including the Tokyo Youth Club administered by the Minato Net 21 (a non-profit organisation in Tokyo), Tohoku University Hospital (Sendai at-risk mental state [ARMS] and first episode service), the University of Toyama Hospital (consultation and support service in Toyama), the University of Tokyo Hospital, Osaka University Hospital, Kochi Medical School Hospital, and the Tokyo Metropolitan Matsuzawa Hospital (Wakaba). The background and present situation of early psychiatric intervention in Japan have been detailed elsewhere.6,7
Practices at the Toho University Omori
Medical Center
The Toho University Omori Medical Center is located in Ota, a city with a population of about 700,000 located in the southern area of the Tokyo Metropolitan region. Our department is named the ‘Mental Health Center’ to avoid the stigma of psychiatry and mental disorders. About 150 outpatients visit the department each day. Having 2 psychiatric wards — a closed ward with 18 beds and an open ward with 18 beds, the Center serves psychiatric patients with physical problems as well as regular psychiatric patients. Therefore, our department shoulders the responsibility of being a core institution for mental health care in the area. The strengths of our department are early intervention for young people and cognitive rehabilitation, which are practised at the Youth Clinic and at Il Bosco, a special day-care service. We aim at establishing a multi-dimensional treatment centre for early psychosis that encompasses symptom reduction, cognitive function, social functioning, quality of life, psycho-education, and family intervention.8
Youth Clinic
As part of the worldwide trend toward early psychiatric intervention, a Youth Clinic specialising in the treatment of young individuals with an ARMS was established in our department in 2007. The PRIME Screen-Revised test (PS-R)9 is administered to all first-time patients younger than 40 years to screen for ARMS as part of the routine preliminary examinations. The PS-R is a self-reported screening test that consists of 11 items regarding attenuated psychotic symptoms and only requires 5 minutes to complete. Patients with positive PS-R results or who are suspected of having ARMS after an examination are introduced to the Youth Clinic, where they are interviewed for diagnostic purposes using the Structured Interview for Prodromal Syndromes / Scale of Prodromal Symptoms, Japanese version.10 They are also supposed to undergo neuroimaging and cognitive testing for detailed examination. When a patient is found to meet the criteria for ARMS, treatment such as stress management, coping strategies for psychotic symptoms, and problem-solving skills is started. Medication with low-dose antidepressant, minor tranquilizer, or major tranquilizer might also be considered.
Il Bosco
Day-care Service for Patients with Early Psychosis
To develop early intervention in Japan and put it into practice, the conventional day-care service intended mainly for patients with chronic schizophrenia was terminated. In May 2007, a new day-care service, which specialises in the care and support of individuals with ARMS or first-episode psychosis aged 30 years or younger, was established. The service unit, named Il Bosco, aims at providing early intervention to prevent the development of full-blown psychosis in ARMS patients, as well as intensive rehabilitation to enable first-episode schizophrenia patients to return to the community.7 The staff members consist of a variety of professionals, including psychiatrists, nurses, occupational therapists, clinical psychologists, social workers, and pharmacologists. The registration period is limited to 1 year for concentrated care in principle, and can be extended up to 2 years depending on the patient’s condition. Adequate medication is offered at the Youth Clinic, and intensive psychosocial treatment is provided at Il Bosco. The contents of the daily programmes are specifically considered with the intention of promoting the brain plasticity of young patients and providing an environment and atmosphere where patients can feel relieved without stigma.
Approaches and Programmes
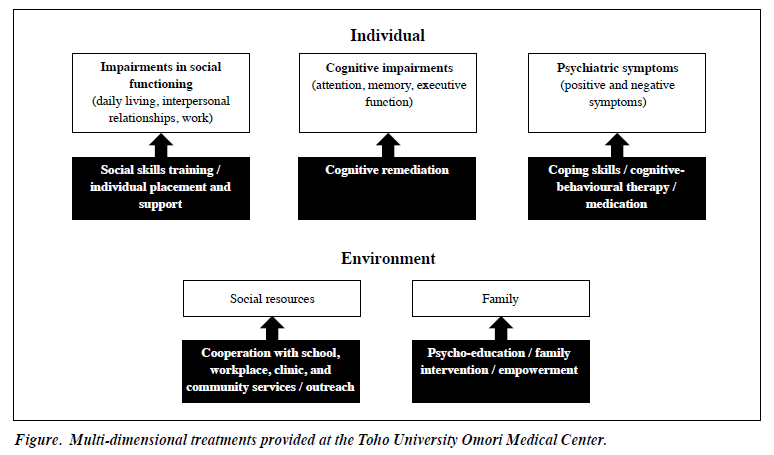
A comprehensive support system suitable for targeted generations is indispensable to the success of psychiatric rehabilitation, and multiple and integrated approaches are administered based on the Optimal Treatment Project11 at Il Bosco, in collaboration with the Youth Clinic (Fig). We offer programmes for learning and training in interpersonal relationships using worksheet and role-playing activities, practices for daily living skills such as cooking, study time for patients to keep up with their friends at school, patient- managed meetings to promote responsibilities and roles within a group, family intervention and psycho-education, as well as group therapy. We sometimes address the stigma of mental illness in the education programme.
The creation of patient goals and plans to accomplish these goals carefully and quickly is vital during the introduction period, because delays can lead to a widening distance from the community and seem to create an inferiority complex or despair, especially among adolescents. Goals can also foster hope regarding an individual’s prognosis and can motivate them to join programmes. Speed is requested in every situation at Il Bosco. Young patients need to start to make a return to the community early, because they usually wish to keep their previous role in the community. Therefore, the contents of each programme must be subdivided, and frequent interviews are necessary to respond to their needs individually. We sometimes offer special programmes to only a few patients who require such programmes. Our aim is for patients to be stable not only in the day-care service unit, but also in the community.
Supporting and paying attention to patients who are building interpersonal relationships within the service is also important because young patients often quickly approach other patients in the same generation using cell phones and emails; such relationships can fail because of poor and immature interpersonal relationship skills, although some patients are obstinately hesitant to communicate with others. Efforts to handle this problem may also contribute to the low dropout rate (11.9%) at Il Bosco.
Many patients (60.0%) have achieved their goals within 1 year since the establishment of Il Bosco; such goals include returning to school, transferring to a correspondence course school, starting to go to preparatory school, and beginning an occupation. Although many patients visit to ask for a consultation or to report on their present condition even after they have completed their course, some patients may be caught in a dilemma and may wish to forget their days at the centre. We are presently considering how to continue supporting these patients after they completed the Il Bosco programme.
Cognitive Rehabilitation
At Il Bosco, cognitive remediation, which directly targets brain function in addition to a psychosocial approach, is adopted. Both of these approaches are regarded as wheels in the promotion of early psychiatric intervention. Institutions that adopt such an approach to individuals with early psychosis are still uncommon throughout the world. Cognitive remediation has been in the spotlight as a novel approach to promoting remission and recovery under existing conditions in which medication is not effective for alleviating impairments in social functioning in schizophrenic patients,12 although more empirical research is necessary to confirm the efficacy of cognitive remediation in the early course of schizophrenia.13 Our cognitive remediation programme mainly targets divergent thinking deficits, because it is found that cognitive training for divergent thinking leads to significant improvements in negative symptoms and social functioning of patients.14
Also, broad cognitive rehabilitation programmes are carried out and a suitable approach for young patients, such as outdoor cognitive remediation and combining cognitive remediation with physical exercise, is devised.15
Collaboration with Community Resources
We are actively engaged in activities to enlighten the community and to disseminate information on the prevention of mental disorders and to reduce the stigma associated with mental disorders. We distribute booklets and leaflets on early psychosis described in an easy and open- minded style to people in the field of education as well as to patients and their families, since collaborating with them is important for achieving early intervention. We also have many opportunities to collaborate with nursing teachers. Young people tend to stay away from medical services because of uneasiness. Therefore, a self-check sheet is offered to allow individuals to contemplate their mental condition. In addition to providing a means of introducing individuals who need help to appropriate psychiatric services, accurate psychiatric information is also available on the Il Bosco website (http://www.lab.toho-u.ac.jp/med/ omori/mentalhealth/). Importantly, we focus not only on psychiatric symptoms, but also on patients’ difficulties in daily living when starting the interventions.
Future Prospects
At present, we provide the same programmes both for individuals with first-episode schizophrenia and for those with ARMS at Il Bosco. However, ARMS patients usually maintain better cognition and social functioning than those with first-episode psychosis, and most of them are younger and are students in high school or college. Different approaches may be needed for patients with ARMS and for those with first-episode schizophrenia. More phase-specific and need-specific services will be indispensable for early psychiatric intervention in the future.
References
- OECD Health Data 2009. Paris: Organisation for Economic Co- operation and Development; 2009.
- McGorry PD, Nelson B, Amminger GP, Bechdolf A, Francey SM, Berger G, et al. Intervention in individuals at ultra-high risk for psychosis: a review and future directions. J Clin Psychiatry 2009;70:1206-12.
- Yamazawa R, Mizuno M, Nemoto T, Miura Y, Murakami M, Kashima H. Duration of untreated psychosis and pathways to psychiatric services in first-episode schizophrenia. Psychiatry Clin Neurosci 2004;58:76-81.
- Yamazawa R, Nemoto T, Kobayashi H, Chino B, Kashima H, Mizuno M. Association between duration of untreated psychosis, premorbid functioning, and cognitive performance and the outcome of first- episode schizophrenia in Japanese patients: prospective study. Aust N Z J Psychiatry 2008;42:159-65.
- Nishii H, Yamazawa R, Shimodera S, Suzuki M, Hasegawa T, Mizuno M. Clinical and social determinants of a longer duration of untreated psychosis of schizophrenia in a Japanese population. Early Interv Psychiatry 2010;4:182-8.
- Mizuno M, Nemoto T, Tsujino N, Funatogawa T, Takeshi K. Early psychosis in Asia: insights from Japan. Asian J Psychiatry 2012;5:93-7.
- Mizuno M, Suzuki M, Matsumoto K, Murakami M, Takeshi K, Miyakoshi T, et al. Clinical practice and research activities for early psychiatric intervention at Japanese leading centres. Early Interv Psychiatry 2009;3:5-9.
- Penn DL, Waldheter EJ, Perkins DO, Mueser KT, Lieberman JA. Psychosocial treatment for first-episode psychosis: a research update. Am J Psychiatry 2005;162:2220-32.
- Kobayashi H, Nemoto T, Koshikawa H, Osono Y, Yamazawa R, Murakami M, et al. A self-reported instrument for prodromal symptoms of psychosis: testing the clinical validity of the PRIME Screen-Revised (PS-R) in a Japanese population. Schizophr Res 2008;106:356-62.
- Kobayashi H, Nozaki S, Mizuno M. Reliability of the Structured Interview for Prodromal Syndromes Japanese version (SIPS-J) [in Japanese]. Jpn Bull Soc Psychiat 2007;15:168-74.
- 1 Falloon IR, Montero I, Sungur M, Mastroeni A, Malm U, Economou M, et al. Implementation of evidence-based treatment for schizophrenic disorders: two-year outcome of an international field trial of optimal treatment. World Psychiatry 2004;3:104-9.
- Medalia A, Choi J. Cognitive remediation in schizophrenia. Neuropsychol Rev 2009;19:353-64.
- Barlati S, De Peri L, Deste G, Fusar-Poli P, Vita A. Cognitive remediation in the early course of schizophrenia: a critical review. Curr Pharm Des 2012;18:534-41.
- Nemoto T, Yamazawa R, Kobayashi H, Fujita N, Chino B, Fujii C, et al. Cognitive training for divergent thinking in schizophrenia: a pilot study. Prog Neuropsychopharmacol Biol Psychiatry 2009;33:1533-6.
- Nemoto T, Mizuno M. Improvements in spontaneity and social functioning in patients with schizophrenia after cognitive training [in Japanese]. Seishin Shinkeigaku Zasshi 2011;113:374-9.
