
Hong Kong J Psychiatry 2001;11(3):2-6
ORIGINAL ARTICLE
Z Feng, H Tian, J Liu
Dr Z Feng, MD, Chief Psychiatrist, Director of Psychiatric Laboratory, Tianjin
Anding Hospital, and Professor, Tianjin Medical University, Tianjin, China Dr H Tian, MD, Visiting Psychiatrist, Tianjin Anding Hospital, Tianjin, China Dr J Liu, MD, Deputy Chief Psychiatrist, Tianjin Anding Hospital, Tianjin, China
Address for correspondence: Dr Z Feng, Tianjin Anding Hospital,
39 Wujiayao Street, Hexi District, Tianjin 300074, China. Tel: (86 22) 2361 6337 (private); (86 22) 2351 6975 (office) Fax: (86 22) 2337 1244
Submitted: 1 March 1998; Accepted: 10 January 2001
Abstract
This paper reports the clinical characteristics of patients with Turner’s syndrome and mental disorder, as evidenced by 5 patients managed at the Tianjin Anding Hospital, along with 12 patients reported in the Chinese medical literature. Schizophreniform psychosis was the most common psychiatric diagnosis made, while presentation resembled bipolar affective disorder in a smaller number of patients. The aetiology, typology, and treatment of this disorder is outlined. The importance of recognising characteristic physical features of Turner’s syndrome in the psychiatric clinic in order to reach a definitive diagnosis and implement appropriate psychiatric treatment is highlighted.
Key words: Chromosome abnormalities, Gonadal dysgenesis, Karyotyping, Mental disorders, Turner’s Syndrome
Introduction
Turner’s syndrome is also referred to as congenital ovarian agenesis. The typical chromosome karyotype is 45,X. Some studies have repor ted that patients with 1 surplus X chromosome (Klinefelter’s syndrome) frequently have associated mental and behavioural disorders.1-3 Patients with Turner’s syndrome suffering from mental disorders have been reported sporadically in the literature. In the past, these patients have often been misdiagnosed with schizophrenia or affective disorder.4-9 In order to investigate the clinical characteristics of patients with Turner’s syndrome and mental disorder, the details of 5 patients managed at the Tianjin Anding Hospital are reported, along with f indngs in 12 patients reported in the Chinese medical literature.4,6,7-13
Clinical Features
General Information
Five patients with Turner’s syndrome and mental dis- orders were identif ied among patients seen at the Tianjin Anding Hospital. They were examined by 2 psychiatrists during their hospital stay and underwent routine labora- tory tests, standard neuropsychological examinations, gynaecological examination, X-ray and B-mode ultrasonic scanning studies, electroencephalography (EEG), and dermatoglyphic and cytogenetic tests. Information on the other 12 patients was obtained from Chinese medical literature sources. All patients met the International Classification of Diseases Tenth Revision (ICD-10) criteria for Turner’s syndrome. They were all Chinese people of the Han race.
All 17 patients were of female phenotype. Mean age at onset of mental disorder was 21.5 years (range 17 to 38 years, SD, 6.6 years). The mean age at which a def initive diagnosis was made was 23.8 years (SD, 6.6 years), meaning that, on average, diagnosis was determined 2.3 years after onset. Mean duration of mental illness was 2.7 years (range, 1 month to 8 years, SD, 2.6).
Among the 15 patients treated in hospital, 8 were diagnosed with schizophrenia, depression, or reactive psychosis, while the remaining 7 were diagnosed with mental disorder secondary to Turner’s syndrome. Two further patients were treated in the outpatient department. Three patients had been married, but were infertile. None of their parents or grandparents had a history of sibling marriage. One patient had a cousin of short stature, and one a grandmother and an aunt with a history of psychosis.
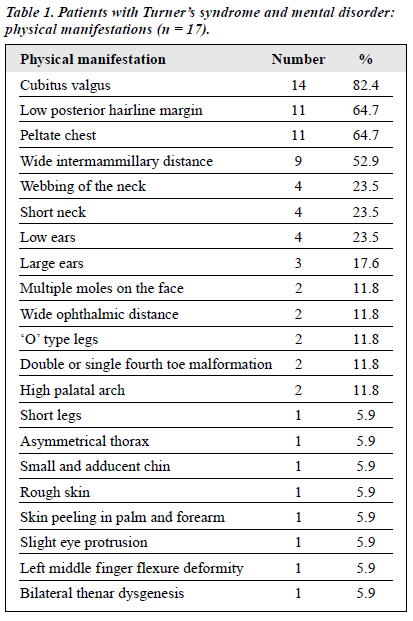
Physical Manifestations
The majority of patients were of short stature. Mean height for the group was 1.38 m (range, 1.24 to 1.40 m, SD, 0.06 m). Mean weight of the patients was 36.9 kg (range, 24 to 48 kg, SD, 8 kg). Other physical manifestations identif ied in this group of patients are summarised in Table 1.
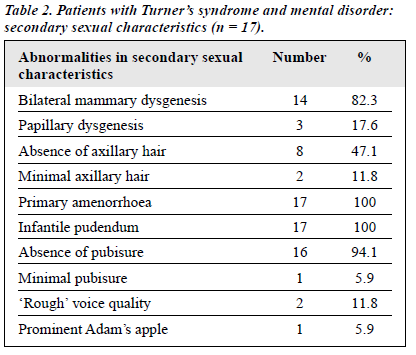
Secondary Sexual Characteristics
Abnormalities in secondary sexual characteristics identified among the patients are listed in Table 2. Gynaecological examination and B-mode ultrasonic scanning of 1 patient showed that the vagina was short and narrow. Of 16 patients in whom the uterus was examined by ultrasound, 15 showed uterine agenesis with the uterus resembling a strip, broad bean, peanut, or soybean in appearance. Investigation of the ovaries of 11 patients found the ovaries to be either absent or strip-shaped.
Personality Features and Personality Tests
Clinical observation suggested that 15 patients were introverted, while 9 were reportedly unsociable and eccentric. Two patients appeared timid, while excess suspicion, sensitivity, and impulsiveness was noted in a further 3 patients, respectively. The Minnesota Multiphasic Personality Inventory (MMPI-2) was completed by 2 patients and the Rorschach test by a further 1 patient, indicating serious personality defect or mental disorder in each patient.
Intellectual Development
All patients were born following a normal pregnancy and delivery. Eleven patients were noted to have been delayed in speech and motor development. Nine patients demon- strated poor academic performance in school, failing a number of subjects, or having to repeat grades. The majority of patients either failed to graduate from primary school, or discontinued junior middle school because of poor intel- lectual performance.
Ten patients were tested with the Wechsler Adult Intelligence Scale-Revised (WAIS-R). The intelligence quotient (IQ) ranged from 46 to 86, with a mean of 68.5 (SD, 12.4). Mean verbal IQ was 76.8 (SD, 15.9). The mean performance IQ score of 57.8 (SD, 13.4) was similarly lower than nor mal. One patient was found to have nor mal intelligence, while the remaining 9 presented with varying grade for 4, and moderate for 1).
Radiological and Other Investigations
Cranial computed tomography was completed for 5 patients and showed no abnormalities. Eleven patients had chest radiographs, of which 3 showed abnormalities — ‘S’ type deformation of the thoracic spine, secondary delayed closure of the ossification centre, mild enlargement of the left cardiac ventricle, widened aortic shadow, and stronger pulsation of the aorta. In 3 patients whose extremities were examined by X-ray, 1 was found to have osteoporosis of the phalanges, a short and rough f irst tarsus in both feet, long and short bone dysostosis, and delayed closure. In another patient phalangeal deformity and epiphyseal immaturity were found. A further patient, 23 years old, was found to have a long bone age equivalent to a 16-year-old. Electrocardiography (ECG) was completed for 13 patients, with 3 showing sinus tachycardia and 1 for associated with high voltage in the left ventricle. EEG examinations of 10 patients showed low voltage in 1 and slow alpha rhythm as well as scattered theta activities in another.
Dermatoglyphic Findings
Twelve patients were examined for dermatoglyphic features. Nine (75%) demonstrated a simian line (the population prevalence of this feature is 9 to 10%), and t’ shifted to the centre of both palms (became t). Most of the atd angles were larger than 40º, and 2 were larger than 60º. Total finger ridge count showed an evident increase, the mean score being 179.3 (SD, 17.7), while the mean score in a healthy population is approximately 138. The highest individual score was 205. The a-b ridge count was 85 in 1 patient, compared with a normal count of approximately 38.
Cytogenetics
Sex chromatin was absent for 2 patients. Various karyotypes identified in the peripheral blood of the 17 patients were seen: 45,X/46,XX in 8 (47.1%); 45,X in 4 (23.5%); 46,Xi (Xq) in 2 (11.8%); 45,X/46,Xi (Xq) in 2 (11.8%); and 45,X/46,XY in 1 (5.9%).
Precipitating Causes and Clinical Features of Mental Disorders
Among 15 cases with adequate history, 10 had apparent precipitating causes (66.7%). The onset in 9 appeared to be related to negative responses from the community to their defective development. They reportedly felt inferior due to lack of menstruation or diff iculty in having sexual intercourse. In 14 patients, the mental disorder presented with a schizophrenia-like psychosis.
The majority of the patients exhibited behavioural disorders. Hallucinations (mostly auditory and visual) and delusions (mostly of reference and persecution) were found, as well as disordered thinking, apathy, inappropriate giggling and muttering to themselves, and irritability. Three patients presented with manic-depressive symptoms, 2 of whom showed depressive mood, paucity of speech, pessimism, weeping episodes, anxiety, anorexia, loss of interest in activities, and suicidal tendency. The onset for the third patient was acute, with symptoms including agitation, over- excitement, and incessant speech.
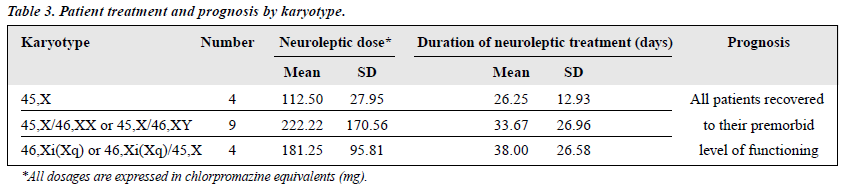
Treatment and Effect
All 17 patients were treated with antipsychotic agents — chlorpromazine (11), perphenazine (3), clozapine (1), sulpiride (1), and taractan (1), These agents were used in low or moderate dosages (Table 3). For 4 patients, this treatment was combined with amitriptyline, oestrogen, thyroxine, or nandrolone in each respective case. Thirteen patients received inpatient treatment, generally lasting between 1 and 4 weeks. Mental disorders subsided with treatment, and all patients returned to their premorbid level. Nine patients were reviewed periodically for 1 to 2 years and remained well without relapse.
Discussion
Turner’s syndrome is characterised by the 45,X karyotype. The incidence of this sex chromosome abnormality in the general population is about 1 in 3000.14 Patients with this karyotype may have been identif ied more readily than those with other genetic abnormalities since genetic investigations have been more commonly undertaken in psychiatric clinics. Approximately 51% of patients with Turner’s syndrome are estimated to be homozygous (45,X), 18% heterozygous or showing mosaicism, while approxi- mately 25% of patients show an abnormal X chromosome structure.15
In the current series of patients, only 4 were found to have the 45,X karyotype, while the remainder demonstrated mosaicism or the X isochromosome type. This suggests that mental disorders are more common in individuals with Turner’s syndrome of the heterozygote genotype.
Aetiology of Mental Disorders
Psychosocial Factors
Gonadal dysgenesis, endocrine disorder, and the lack of secondary sexual characteristics, affect both psychological and personality development in individuals with Turner’s syndrome. Most of the patients in the current group were introverted, demonstrating solitary, passive behaviour and a lack of impulse control. A negative self-image and poor self esteem were also common features.
Nine patients were very concerned about their short stature, amenorrhoea, and lack of feminine characteristics, which led to shame and belittlement. Six reported envy of other women or their female siblings’ heterosexual relationship and marriage. Negative personality traits appeared to undermine normal psychological defence mechanisms. Moreover, socialisation in general was an area of weakness, especially with respect to coping skills, because of the patients’ low intelligence.5
Downey et al compared 23 women with Tur ner’s syndrome with their normal sisters and other women of similar physique and short stature.16 These investigators reported that the overall mental functions of patients with Turner’s syndrome were impaired, and they were socially disabled. These authors infer red that patients with Turner’s syndrome were prone to develop mental disorders when faced with the stress of more frequent social acti- vities after puberty, since they were likely to adapt with diff iculty.
Biological Factors
Patients in the current study had f indings in keeping with impaired brain development. The majority demonstrated delayed development of speech and motor skills in their childhood. One of 10 patients assessed by EEG showed slow alpha rhythm and scattered theta activities. Bone dysgenesis, delayed closure of the epiphysis, phalangeal deformity, and dermatoglyphic alterations were seen in some patients.
Of note, both skin and the nervous system arise from the endoblast during embryonic development. Steffen et al reported the results of neuropsychological evaluation of 18 patients with Turner’s syndrome, aged between 5 and 15 years.17 Fourteen patients demonstrated the neuropsycho- logical syndrome of delayed right hemispheric maturation, manifested by complex stereognostic diff iculties and confusion of body image, whereas this syndrome is seen in only approximately 2% of the general population.
Furthermore, it is thought that as a result of ovarian agenesis, endocrine def iciencies, and dysgenesis of secondary sexual characteristics, the function of the gonado- hypophysio-hypothalamic axis might be disturbed, resulting in a decrease in oestrogen levels and, in turn, an elevated gonadotrophin level.18 Some authors, discussing the co- morbidity of Turner’s syndrome and anorexia nervosa, have reported that luteinising hormone levels and follicle stimulating hormone levels were obviously reduced in patients with Turner’s syndrome, and that the patients suffered disordered pituitary function.19,20
Although the prevalence of patients with Turner’s syndrome among females with intellectual deficiency is only 0.64%, one-quarter of patients with Turner’s syndrome are reportedly mentally subnormal.3 In the current sample, 9 of 10 patients tested were found to present with mild or moder- ate grade mental retardation (mean IQ, 68.5). Moreover, performance IQ was more impaired (mean performance IQ, 57.8), consistent with f indings in the literature.3,18 The prevalence of intellectual deficiency was higher overall in the current group of patients, suggesting that patients with Turner’s syndrome and low intelligence are more likely to suffer from mental disorders.
Type of Mental Disorders
The mental symptoms of patients with Turner’s syndrome most frequently resemble those of schizophrenia,4,7,10-13 while a minority present with a manic-depressive type of illness. Most patients, however, lack the typical core symptoms and do not follow the typical course of the disorder — the progressive mental deterioration seen in schizophrenia, or the pattern of remission and recurrence commonly seen in affective disorder. Rather, mental disorder in patients with Turner’s syndrome is similar to the psychiatric attacks seen in patients with mental retardation.
Fishbain and Vilasuso15 and Panzer and Tandon21 have reported individuals with Turner’s syndrome and bipolar affective disorder. Both patients had a family history of bipolar affective disorder, although this may be a coincidental f inding.
In the current study, patients with Turner’s syndrome and an associated mental disorder were categorised as having a schizophreniform type or manic-depressive type illness, according to clinical features. The main clinical features of the schizophreniform type illness included behavioural disturbance, hallucination, delusion, thought disturbance, and irritability. Clinical manifestations of the manic-depressive type illness observed were similar to either the manic or depressive phase of an affective disorder.
Treatment
Generally speaking, low dosage medications and short-term treatment have been shown to be effective for mental illness associated with Turner’s syndrome. It is not necessary to use antipsychotic agents in high doses for lengthy periods, or to use electroconvulsive therapy. Antipsychotics, antidepressants, or tranquilizers can be selected according to the presenting symptoms. Some authors have suggested that the therapeutic effect of treatment can be improved by adding oestrogen to the regimen.11,12 Ostrogen in low doses may be added, but should not be used for a prolonged period of time, and can be gradually discontinued upon remission of the psychiatric symptoms.
It is very important to also assist patients in recognising and accepting the consequences of Turner’s syndrome, as this can improve psychological stamina. Ideally, if we could identify patients with Turner’s syndrome in childhood, provide them with psychotherapy and endocrine replacement therapy early on, and offer special education to those patients with learning disabilities, the occurrence of mental disorders might be reduced in this patient group.
Physical Characteristics Assist Diagnosis
The main features of Tur ner’s syndrome are ovarian dysgenesis, absence of female sexual characteristics, and primary amenorrhoea. The syndrome is often associated with short stature and other abnormalities in physical appearance, including a small chin, low ears, low posterior hairline margin, webbing of the neck, peltate chest, wide inter- mammillary distance, and cubitus valgus. Rectoabdominal examination reveals a very small or absent uterus. B-mode ultrasonic scanning indicates dysgenesis of the uterus and ovaries. Key dermatoglyphic features of this patient group are a higher frequency of the simian line, dot t shift to the centre of the palm, increased atd angle, and increased total f inger ridge count. EEG examination may show slow alpha rhythm and scattered theta activities.
On encountering such abnormalities in a patient with symptoms resembling schizophrenia or affective disorder in the psychiatric clinic, prompt cellular genetic examination should be arranged. This involves assessment of the sex chromatin in cells of the buccal musosa, as well as the karyotype in peripheral blood. By identifying patients presenting with mental illness who have Turner’s syndrome, more appropriate care can be provided, and prolonged use of unnecessarily high doses of antipsychotic drugs can be avoided.
References
- 1. Shinichiro N. A cytogenetic and genetico-epidemiological study of mental disorders. Psychiatria Neurologia Japonica 1983;85:207-214.
- Feng ZY. The mental and behavior disorder of patients with sex chromosome anomaly. Foreign Med Sci Ref J Psych 1984;11:148.
- Feng ZY, Ma JQ, Li HY, et al. A study of the sex chromatin fre- quency in patients with mental disorders. Chin J Neurol Psychiatry 1992;25:306.
- Yu L, Hu L. A report of 1 case with Turner’s syndrome and schizo- phrenia. The Information of the First Psychoneurosis Genetics Meeting in China;1981:1-6.
- Feng ZY. A report of 4 cases with mental disorder and sex chromosome abnormality. Tianjin Med J 1986;14:282-285.
- Wu JW, Wu BQ, Zhang H. A report of 1 case with Turner’s syndrome and mental disorder. Chin J Neurol Psychiatry 1983;9:94.
- Zhao LR, Yan JX. A report of 1 case whose karyotype was 45,XO associated with mental disorder. J Hebei Ment Health 1993;6:38.
- Wang YQ. A report of a woman with genitalia dysgenesis and mental disorder. J Hebei Ment Health 1994;7:26.
- 9. Hong H. A report of 1 case with Turner’s syndrome and mental disorder. J Hebei Ment Health 1995;8:162.
- Wang SH, Wu LX. A report of 1 case with Turner’s syndrome and mental disorder. The Information of the Second Psychoneurosis and Genetics Meeting in China; 1985:1-3.
- Zhang L, Zhang L, Jia YC. Schizophreniform manifestation in Turner’s syndrome. Chin J Neurol Psychiatry 1983;9:81.
- Wang SY, Jiang H. A report of 1 case with Turner’s syndrome and mental disorder. J Hebei Ment Health 1995;8:92.
- Wang XP, Wang GH, Liu XP, et al. A report of 2 cases with Turner’s syndrome and mental disorder. J Hebei Ment Health 1996;9:212.
- Shinichiro N. Symptoms of sex chromosome anomaly. Jap J Clin Psych 1985;14:674-678.
- 15. Fishbain DA, Vilasuso A. Manic-depressive illness associated with Turner’s syndrome mosaicism. J Nerv Ment Dis 1981;169:459-461.
- Downey J, Ehrhardt AA, Gruen R, Bell JJ, Morishima A. Psycho- pathology and social functioning in women with Turner’s syndrome. J Nerv Ment Dis 1989;177:191-201.
- Steffen H, Heinrich U, Kratzer W. Stereognostic difficulties. A syndrome of delayed right hemispheric maturation [article in German]. Kinder Jugend Psych 1978;6:131-141.
- Akio A. Sex chromosome abnormality with mental disorder. Jap J Clin Psych 1980;9:163.
- Kauli R, Gurewitz R, Galazer A, Prager-Lewin R, Gil-Ag I, Laron Z. Effect of anorexia nervosa on gonadotrophin secretion in a patient with gonadal dysgenesis. Acta Endocrinol (Copenh) 1982;100:363-368.
- Ohzeki T, Egi S, Kagawa J, et al. Prolonged suppression of gonadotropin secretion after weight recovery in an anorectic patient with Turner’s syndrome: reduced gonadal function in anorexia nervosa is independent in part on nutrition. Horm Metab Res 1989;21:626-629.
- Panzer MJ, Tandon R. Bipolar disorder associated with Turner’s syndrome. J Nerv Ment Dis 1991;179:702.
