J.H.K.C. Psych. (1993) 3, 39-42
ORIGINAL ARTICLE
Summary
The regional cerebral blood flow (rCBF) pattern is a reflection of neural activity in different brain regions due to the tight coupling between regional cerebral blood flow and neuronal activity. With Single Photon Emission Computed Tomography (SPECT) using the flow tracer Tc-99m-HMPAO, high resolution rCBF images can be obtained. SPECT images of five parents with various degree of cognitive impairment and features of dementia are reported. Different rCBF patterns are noticed in Alzheimer’s disease and multi-infarct dementia. The clinical applications of SPECT in the management of dementia are discussed.
INTRODUCTION
Single Photon Emission Computed Tomography (SPECT) is an imaging technique of brain function and is a measurement of regional cerebral blood flow (rCBF). It is based on the observation that there is a tight coupling be tween CBF and metabolic activity. It involves injection of radiopharmaceuticals into a subject and the detection of its distribution by a rotating gamma camera. The gamma camera consists of a collimator (a focusing device),a crystal (sodium iodide) which will emit photons on impact by gam ma rays from radioisotopes and a circuitry that detects and analyses the photon emission pattern. Radiopharmaceutic als commonly used are Tc-99m-HMPAO and 1-123-IMP. These lipophilic isotopes once taken up by the neurons will be transformed to a lipophobic ligand and will stay in the cells. In other words, the pattern of the distribution or radioactivity will be determined by the pattern of regional cerebral blood flow at the time of the injection of radiopharmaceuticals. The patient can be at a resting posi tion during injection or he or she can be asked to perform a variety of tasks like verbal fluency activation as well as pharmacological activation and sensory stimulation (De vous, 1989; Friberg, 1989).
The evolution of various techniques of cerebral blood flow measurement like Positron Emission Tomography (PET) and SPECT and their application in the studies of dementia was discussed by Bonte et al (1990). Brain SPECT is generally regarded as the culmination of a series of investigations of CBF pioneered by Kety and Schmidt (1948). The relative inexpensiveness and simplicity in op eration as compared with PET has made SPECT widely applied in clinical practice. A number of SPECT studies have now been performed using Tc-99m-HMPAO to in vestigate dementia and has been reviewed by Geaney and Abou-Saleh (1990). These studies have shown that SPECT can reveal cerebral abnormalities when CT and MRI do not because the latter are measures of cerebral structure while the former are measures of cerebral function. Various rCBF patterns have been reported in different demented condi tions like Alzheimer's disease (AD), multi-infarct dementia (MID), Pick's disease and Huntington's disease with diffe rent degree of specificity.
The aim of this study is to summarize our experience at Queen Mary Hospital in the SPECT brain imaging of pa tients with various demented conditions and to discuss the relevant clinical applications in psychiatry.
PATIENTS & METHOD
Two patients with Alzheimer's disease, one patient with multi-infarct dementia, one patient with delirium and one patient with depression were studied. The diagnosis in these patients satisfied the DSM-III-R criteria. Mini-Mental State examination (Folstein et al, 1975) was also per formed.
SPECT were performed in the first hour following the in travenous injection of 550MBq of Tc-99m-HMPAO. Injec tion was given within 30 minutes of preparation of the compound. The patient was imaged on a tomographic table using a rotating gamma camera (Elscint Apex). A head support was used that enables the camera to rotate with the minimum possible radius around the patient's head. Images were acquired for 25 seconds each at 60 angles over 360 degrees and the total study time was approximately 30 minutes. A low energy high resolution collimator was used and images structured in a 64 x 64 matrix. A previously acquired SO-million-count flood study was used to correct the acquired data for camera non uniformity. Image reconstruction was achieved by a filtered back-projection process (Metz filter) and multiple transverse image slices were produced. Attenuation correction was done using Chang's method's.
For clinical interpretation, 15 contiguous sections were photographed, parallel to the orbitomeatal line. These im ages in the transverse section file were normalised and dis played sequentially on a colour monitor. Sagittal and coronal slices were reconstructed from the transverse slices and displayed as well. The images were visually inspected and reported. Relevant images from this file were selected and stored in a single 512 x 512 pixel image on hard disk for subsequent analysis.
RESULTS
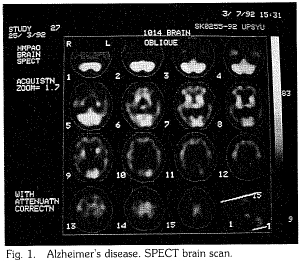
Case 1 M/58 Alzheimer's disease
The retired film producer developed gradual deterioration of memory and speech for 5 years and had to be institutionalised in elderly home. MMSE score was 0/30. CT scan of brain showed cerebral atrophy but was commented by experienced radiologist as within normal limit. SPECT scan of brain showed generalised symmetrical perfusion deficits over the frontal, parietal, temporal and occipital cortices. The hypoperfusion is most marked at the posterior parietal regions (Fig. 1).
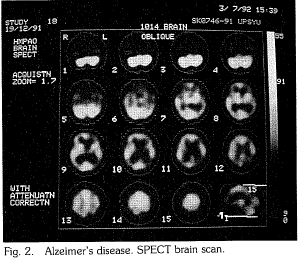
Case 2 F/60 Alzheimer's disease
The retired accounting clerk became increasingly forgetful and irritable for 9 months and there was deterioration in self care. MMSE score was 18/30. EEG was normal. CT scan of brain showed borderline cerebral atrophy. SPECT brain scan showed hypoperfusion over the posterior parietal, temporal and occipital cortices. There was no perfusion deficits at the frontal and anterior parietal regions (Fig. 2).
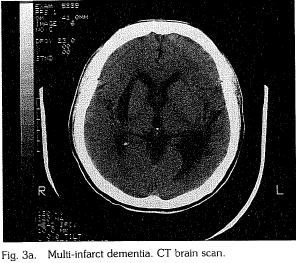
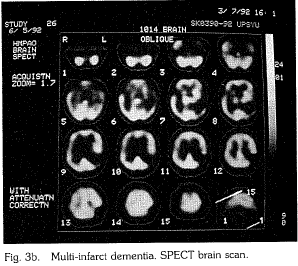
Case 3 F/45 Multi-infarct dementia
The housewife survived two episodes of cerebrovascular acci dent and developed stepwise deterioration in mental state that in cluded irritability, disorientation, suspiciousness, forgetfulness and nominal aphasia. MMSE score was 10/30. CT scan showed multi ple hypo-dense areas (Fig. 3a). SPECT scan showed correspond ing areas of hypoperfusion at the parieto-temporal cortices on the left and at the temporal cortex, basal ganglion and thalamus on the right (Fig. 3b).
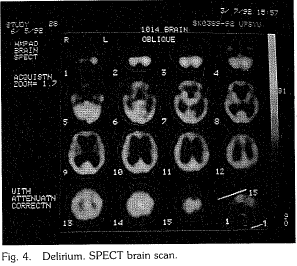
Case 4 F/84 Delirium
The retired domestic worker had history of cancer of breast and received curative mastectomy. She also had diabetes mellitis and her compliance to hypoglycaemic medication was poor. She was noticed to have fluctuating forgetfulness over 6 months with topographic disorientation and deteriorating self care. Her mental state appeared to be related to her diabetes status. She had nor- mal blood sugar level on the day of mental assessment and MMSE score was 25/30. CT scan showed no cerebral atrophy nor evi dence of brain metastasis. SPECT scan of brain was normal (Fig. 4).
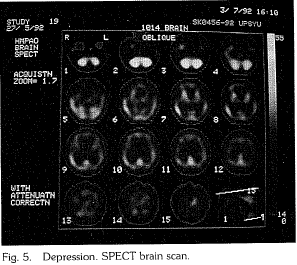
Case 5 F/76 Depression
The anxious housewife who received education up to secondary level had sle.ep problem and became increasingly irritable after sustaining a hip fracture that made her home bound. Her mental state further deteriorated over a year when her husband became indisposed by a cerebrovascular accident. With failing hearing, she was noticed to be confused, sensitive, suspicious and forgetful, Mental examination showed a depressed and irritable lady preoc cupied with her deafness, reduced mobility and failing health. There was no perceptual or thought disorders. She was not moti vated towards cognitive testing and claimed she did not know the answer. However with encouragement and firm handling, she managed to score 24/30 in the MMSE. CT scan of brain was nor mal. SPECT scan of brain showed generalised mild hypoperfusion (Fig. 5)
DISCUSSION
Results from this series of single case study agree with the observation that the use of Tc-99m-HMPAO can be used for differentiating between AD and MID based upon the presence or absence of the characteristic parieto occipital perfusion deficits (Smith et al, 1988). Posterior perfusion deficits have been shown to be a sensitive and specific feature in Alzheimer's disease. Both of our patients with Alzheiner's disease (Case 1 and 2) had this hypoperfu sion. Case 1, who was clinically more demented than Case 2, had a more generalised hypoperfusion pattern than that in Case 2. Whether there is significant correlation between SPECT rCBF pattern and the degree of dementia needs further studies. On the othe.r hand, CT brain scans in both Case 1 and Case 2 remained equivocal in terms of the di agnosis of dementia. This agrees with earlier observations that functional brain imaging is more sensitive and specific than structural brain imaging in the detection of cerebral abnormalities (Geaney and Abou-Saleh, 1990).
Specific patterns are absent in MID as vascular events, unlike degenerative disease which have a predilection for certain brain regions with relative sparing of others, are not consistent in their locus of cerebral damage (Testa et al 1988). Theoretically MID could mimic any findings varying from normal to asymmetrical deficits, However, if an asym metrical pattern is found, affecting areas other than the parietotemporal region, it is suggestive of MID. This im pression is strengthened if the rCBF deficits coincide with cerebral infarcts seen on structural imaging with CT or MRI. This is well demonstrated by the good correlation between the CT brain scan and the SPECT rCBF pattern in Case 3.
Case 4 demonstrates how the assessment of a patient with equivocal clinical picture of dementia can be facili tated with SPECT scan of brain. She had a CT brain scan within the 'normal range of her age' but as discussed above, structural brain imaging is limited by its specificity and sensitivity in the detection of cerebral abnormalities.
On the other hand, as it had been shown that if a patient with clinically apparent dementia has a normal SPECT study it is unlikely to be AD (Geaney an Abou-Saleh, 1990), the normal SPECT brain image in Case 4 can ex clude dementia reliably. This agrees with the clinical picture as the cognitive deficits improve with the control of de lirium after the optimal management of diabetes mellitis.
A rCBF pattern of generalised hypoperfusion that is most marked in the frontal lobes and in basal ganglia has been reported in unipolar depression (O'Connell et al, 1989). Others, however, noted that similar changes are seen in depression as in AD (Upadhyaya et al, 1990). The SPECT brain scan of Case 5 showed mild generalised hypoperfu sion and a borderline cognitive impairment as assessed by the MMSE score. In the presence of depressive symptoms and the absence of the typical posterior hypoperfusion pat tern of AD or the asymmetric hypoperfusion pattern in MID, the diagnosis of depression was made. The cause of the rCBF deficits in major depression is unknown and is unlikely to have a primarily vascular origin as the distribu tion of impaired perfusion does not conform to any topog raphic distribution of the major blood vessels in the brain. Those elderly individuals who present with depression and who have the characteristic AD abnormalities on SPECT might be individuals at risk of developing AD where de pression has been one of the early clinical features. Whether these individuals have a worse prognosis than those with normal SPECT scans remains unanswered until studies of repeat measures or long term follow-up are available. At present, it appears that more work is required to give a definite role of SPECT in the differentiation be tw,2en depression and dementia in the elderly.
As HM-PAO is labelled with Tc, it can be made available to a wider population than PET imaging, being available in all Nuclear Medicine Departments equipped with a tomog raphic gamma camera. SPECT imaging of rCBF will come to play an important role in the diagnosis and management of dementia. The accuracy of clinical diagnosis of AD is of the order of 69% to 87% when correlated with autopsy re sults and it is not unreasonable to suppose that the addition of SPECT rCBF study might improve diagnosis accuracy. More information on the frequency with which perfusion deficits, particularly those with a pattern similar to that in AD, on visual inspection of SPECT studies in healthy, elderly controls would certainly help. Regional cerebral blood flow determination may play a role in identifying pa tients with treatable dementias and it may also be used to screen individuals who are at risk to the familial form of AD. The development of the radioligand 123I-QBN for the study of muscarinic cholinergic receptors in the study of AD (Holman et al, 1985) would also contribute to our understanding of dementias. SPECT can also be applied in the evaluation of experimental drugs that may arrest the progress of AD and perhaps even effect improvement in the patient's clinical state (Bonte et al, 1990). Tc-99m HMPAO imaging should prove useful for aiding in the posi tive diagnosis of dementia of the Alzheimer's type as well as for differentiating it from other dementias. It will also be useful in the management of the elderly depressed patient, in terms of differentiation from dementia and to exclude the presence of cerebral vascular accident when planning electroconvulsive therapy. We believe that HM-PAO imag ing should prove useful in the management of a wide range of neuropsychiatric patients, often by confirming the clinical diagnosis, but also by contributing to patient man- agement in many cases.
REFERENCES
Bonte, F.J., Hom, J., Tintner, R., Weiner, M.F. (1990) Single Photon Tomography in Alzheimer's Disease and the Dementias. Seminars in Nuclear Medicine, Vol. XX, No. 4 (October), pp. 342-352.
Devous, M. (1989) lmaginng brain function by single-photon emis sion computer tomography. In Brain Imaging: Applications in Psychiatry (ed. N. Andreasen), pp. 147-234. Washington DC: American Psychiatric Press.
Folstein, M.F., Folstein, S.E. and Meltryh, P.R. (1975) Mini-mental state - A pract\cal method for grading the cognitive state of pa tients for the clinician. Journal of Psychiatric Research, 12: 189-198.
Friberg, L. (1989) Regional Cerebral Blood Flow in Psychiatry as Measured by Single Photon Emission Computed Tomography. Psychiatry Research, 29: 319-322.
Geaney, D.P.. Abou-Saleh M.T. (1990) The Use and Applications of Single-Photon Emissin Comuterised Tomography in Demen tia. British Journal of Psychiatry, 157 (suppl. 9): 66-75.
Holman, B., Gibson, R., Hill, T., et al (1985) Muscarinic acetylcho line receptors in Alzheimer's disease: in vivo imaging with iodine 123-labeled 3-quinuclidinyl-4-iodobenzilate and em1ss1on tomography. Journal of the American Medical Association, 254: 3063-3066.
Kety, S.S., Schmidt, C.F. (1948) The nitrous oxide method for quantitative determination of cerebral blood flow in man: Theory, procedure and normal value. Journal of Clinical Inves tigation, 27: 476-483.
O'Connell, R.A., Van Heertum, R.L., Billick, S.B. et al (1989) Single photon emission computered tomography (SPECT) with I-123-IMP in the differential diagnosis of psychiatric disorders. Journal of Neuropsychiatry, I: 145-153.
Smith, F.W., Besson, J.A.O., Gemmell. H.G., Sharp, P.F. (1988) the Use of Technetiu,-99m-HM-PAO in the Assessment of Pa tients with Dementia and Other Neuropsychiatric Conditions. Journal of Cerebral Blood Flow and Metabolism, 8, Suppl. 1: 116-122..
Testa, H.J., Snowden, J.S., Neary, D., Shields, R.A., Burjan, A.W.I., Prescott, M.C., Northen, B., Goulding, P. (1988) the Use of [99m-Tc]-HM-PAO in the Diagnosis of Primary Degenerative Dementia. Journal of Cerebral Blood Flow and Metabolism, 8, Suppl. 1: 123-126.
Upadhyaya et al (1990) not provided by author. (Ed.)
*Michael T.H. Wong MBBS, MRCPsych. Lecturer, Department of Psychiatry, University of Hong Kong.
Henry W.P. Yeung MBBS, FRCR, DipABIM. Consultant, Department of Nuclear Medicine, Queen Mary Hospital.
*Correspondence: Neuropsychiatry and Epilepsy Unit. The Maudsley Hospital, Denmark Hill, London SES 8AZ, United Kingdom. 50