Hong Kong J Psychiatry 2001;11(1):12-16
REVIEW ARTICLE
E Cocks
Abstract
Following a brief account of 3 key aspects of normalisation, this paper describes the key features of social role valorisation and some social role valorisation applications to service development. Normalisation and social role valorisation are widely acknowledged as having strongly influenced reforms to services for people with learning disabilities in many parts of the world. Social role valorisation is a social theory with relevance to a wider group of people who experience social devaluation. The theory is based on an account of the common experiences (wounds) of devalued people and the development of 10 bodies of conceptual and empirical knowledge (themes) that provide explanation for social devaluation and generate strategies to counter it. Finally, the paper describes 2 applications of social role valorisation to service development, a service development and training instrument (programme analysis of service systems’ implementation of normalisation goals) and a framework for describing, evaluating, and planning a human service (model coherency).
Key words: Human services development, Normalisation, Social devaluation, Social role Valorization
Introduction
Since the 1970s, normalisation and social role valorisation (SRV) have had a profound influence on the development of services for people with learning disabilities and other groups of people within human services, including people with psychiatric disabilities and elderly people. To a significant extent, these ideas have provided a foundation for the reform of institutional services and the development of the community living movement for people with learning disabilities in many countries, including the USA, Canada, Scandinavia, the UK, Australia, and New Zealand. As a measure of the importance of normalisation and SRV, in a well-known Delphi study, 178
North American learning disability specialists were surveyed to determine the publications with the most impact during the past 50 years.1 Two publications by Wolfensberger, a key figure in the development of both normalisation and SRV, were ranked first and 17th.2,3 More than 100,000 copies of the first publication have been sold. There are translations of various SRV texts in French, Japanese, Korean, Spanish, and German. In 1999, the National Historic Preservation Trust on Mental Retardation, a consortium of 7 major learning disability organisations in the USA, selected Wolfensberger as one of 35 persons who have made the most significant contribution to learning disability in the world during the 20th century. The purposes of this paper are to describe the key features of both normalisation and SRV and to provide a description of some SRV applications to service development.
NORMALISATION
The normalisation principle emerged from Scandinavia in the late 1960s and was further developed in North America by Wolfensberger.4 By the early 1970s, these ideas were influencing service developments in many parts of the world. Nirje was a key Scandinavian specialist in the early development of normalisation.5 Normalisation largely evolved as a human rights-based, critical reaction to large institutions, the service model that dominated services for people with learning disabilities from the 19th century. Life for people with learning disabilities in such places was very deprived and abnormal compared with the lives of ordinary people. Poor conditions were documented in the literature from the 1960s in many parts of the world. Normalisation simply stated that these people should be enabled to lead lives like those of ordinary people. Note that normalisation did not talk about
‘making people normal’. Amongst others, 3 powerful ideas underpinned normalisation and these contributed to some important service development principles.
THE NORMAL RHYTHMS OF LIFE
Nirje wrote about the importance of people with learning disabilities being given access to the ‘normal rhythms of life’ in stark contrast to the way people lived and worked in institutional settings (Table 1).5 Even nowadays, 30 years after it was written, Nirje’s work remains powerful.
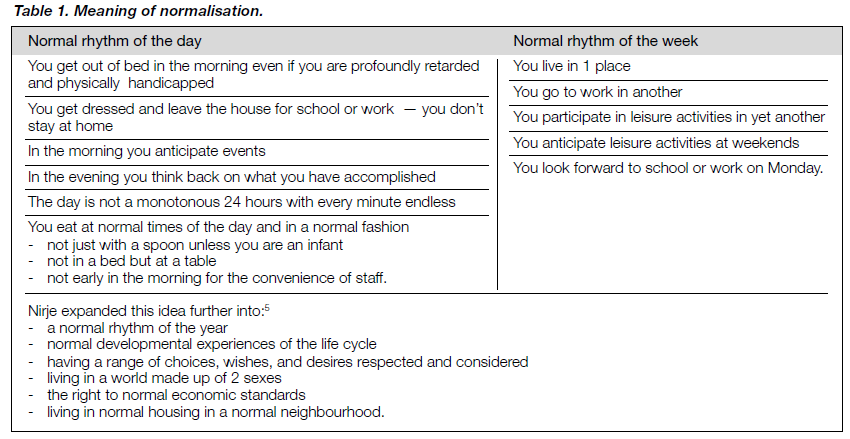
SEPARATION OF LIFE FUNCTIONS
In line with the seminal work of Goffman in his 1968 classic work Asylums, normalisation drew attention to the essential characteristic of institutional life — the fact that almost all life functions are carried out in 1 place, perhaps even in 1 room or ward of an institution.6 In contrast, ordinary valued people experienced ‘separation of life functions’ whereby they might live in 1 place, work in another, be educated somewhere else, and spend leisure time in a variety of places. This provides a richness of experience, relationships, and developmental opportunities that cannot occur if these life functions are concentrated in 1 place.
CULTURALLY VALUED ANALOGUES
Human services usually address the same human needs that all people have such as physical care, a place to live, and opportunities for growth and development, health care, and education. However, the manner in which many services address these needs is very different from the ways in which ordinary valued people have these needs met. The normalisa- tion principle of the ‘culturally valued analogue’ stated that services should be modelled as much as possible on culturally valued ways of addressing the particular needs concerned. This remains an important guiding principle in designing human services, although it is far more common for planners to base services on non-typical models. Clearly, although these ideas are more than 3 decades old and have even longer historical origins, they remain a challenge for human service development.
SOCIAL ROLE VALORISATION
In 1983, following considerable development of the normalisation principle, Wolfensberger suggested a change of terminology to social role valorisation (SRV).3 Although having its origins in normalisation, the extent of development of SRV has meant that it now represents a complex social theory in its own right.
The key features of SRV are as follows:
- SRV is an empirically-based social theory that addresses the social devaluation of individuals and groups. The theory rests on the reality that all human perception is evaluative, especially our perceptions of other people. This means that some individuals and groups are accorded low social value and consequently are vulnerable to social devaluation. The consequences of social devaluation can be described and the factors that contribute to social devaluation can be understood and countered to some extent.
- SRV is relevant to many groups who are vulnerable to, or experience, collective devaluation within different societies and cultures. This includes not only people with learning disabilities, but also other groups of disabled people, people with psychiatric disabilities, elderly people (in many, but not all, cultures), poor people, and people from certain racial and ethnic groups.
- Social devaluation is a social process in which the actual characteristics of the devalued person or group are only 1 influence, and at times even a minor influence. This is because perceptions of others also depend on factors such as previous experience of a certain group of people, personal physical and social conditions (some ethnic groups may be devalued in situations of hardship within a particular social context), and the prevailing societal mores and attitudes towards that group. Perceptions are strongly influenced by historical beliefs and practices towards the group — one of the reasons why some human service practices such as large institutions continue to be so firmly established.
- SRV theory includes a striking phenomenological description of the common life experiences of people who are socially devalued. The theory uses the term ‘wounds’ to describe these experiences and avoids reinterpreting them into professional language such as symptoms. Examples of key wounds include:
- rejection — congregation with ‘their own kind’ and segregated both physically and socially
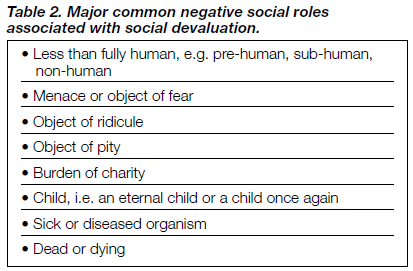
- accorded low social status — cast into one or more devalued social roles (Table 2)
- physical and social discontinuity — being separated from important possessions, places, and relationships
- de-individualisation — loss of positive identity through being subject to mass or institutional regimes and management
- loss — losing control over one’s life, even over the simplest actions
- deprivation — not having access to the ordinary developmental opportunities and experiences of life
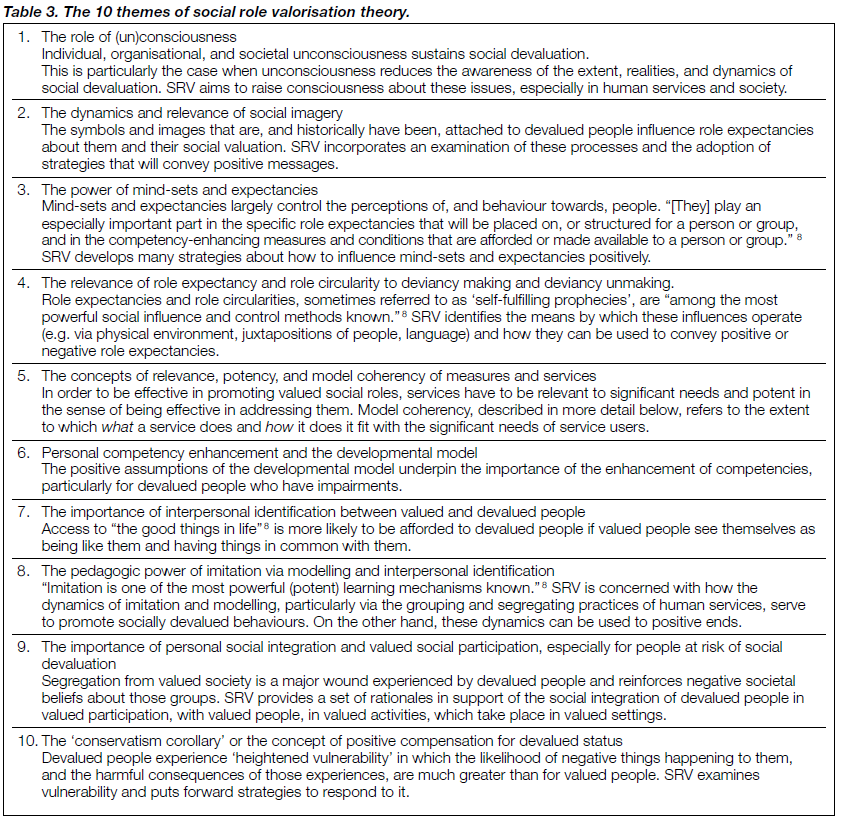
- impoverishment. - The strategic objective set by SRV theory in response to devaluation is to prevent people from being accorded negative social roles in the first place, work to reverse, or at least reduce, the impact of existing negative roles, and promote vulnerable people into positive, valued roles. This can be achieved through 2 key processes: enhancing the social image of vulnerable people and enhancing their competencies. SRV theory then describes 10 themes or bodies of empirical and theoretical knowledge that describe both the dynamics of how and why social devaluation occurs and also provide clear strategies to counter it. These themes are described very briefly in Table 3. More complete accounts can be found in Race7 and Wolfensberger.8
- Because human services are fundamentally a response by societies to groups of socially devalued people, what human services do is of profound importance and influence in regard to both the maintenance of social devaluation and also attempts to counter it.
SRV theory is usually taught over 3 days in work- shop formats that are very systematic and engaging. There is ample literature that describes the theory (including that of Cocks9 and Flynn and Lemay10). Recently, Wolfensberger has articulated the central importance of role theory in SRV and provided examples of the design of practical measures to pursue valued roles for people with learning disabilities.11
APPLICATIONS TO SERVICE DEVELOPMENT
There are many ways in which SRV theory impacts on human service development, not the least being systematic training events that occur regularly in many parts of the world. It is possible to attend such events and information can be sought from the author. Here, 2 specific SRV applications will be briefly considered, the first, a service evaluation instrument, and the second, an approach to describing and analysing a human service programme.
PROGRAMME ANALYSIS OF SERVICE SYSTEMS’ IMPLEMENTATION OF NORMALISATION GOALS
Following the development of ‘programme analysis of service systems’ (PASS),12 an instrument to assess the extent to which a human service programme achieved nor malisation outcomes, a second instrument, ‘programme analysis of service systems’ implementation of nor malisation goals’ (PASSING), was developed to reflect the more recent evolution of SRV theory.13 PASSING is a 42-item rating scale which is structured according to SRV theory. The ratings evaluate what a service does in 4 specific areas that impact on the enhance- ment of service users’ image and on their competencies. The 4 areas are as follows:
- the physical characteristics of the service (e.g. where a service is located and what it looks like inside and out)
- the way the service groups its clients (e.g. size and mix of gender, identities, and needs) and the relationships the service establishes (e.g. between staff and clients)
- the activities in which the service engages the clients, including ‘treatments’ and the extent to which clients’ time is used effectively
- miscellaneous use of language, symbols, and images (e.g. what a service is called and the symbols and images associated with fundraising).
PASSING is used in many parts of the world both as a method of service evaluation and development and in a workshop format to teach people about SRV theory in considerable depth using a practical process that involves evaluating 2 service settings. There have been many PASS and PASSING evaluations since the early 1970s and there is substantial literature that describes these evaluations, establishes the statistical properties of the measures, and draws conclusions about human service quality.9,14,15
MODEL COHERENCY
Model coherency was originally developed by Wolfensberger as a single rating within PASS and has been developed considerably since the 1970s.2,4,8,12 It is now described as one of the themes of SRV theory and is taught in workshop formats. What follows is a brief description of the key features of model coherency.
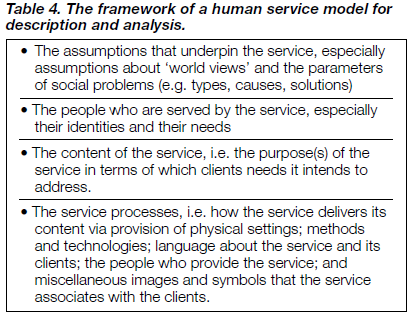
Model coherency uses the framework of a ‘human service model’ (Table 4) which allows description and analysis of any type of human service for any type of client group. Having a universal framework for description lends itself to the additional purposes of designing and planning a new service, evaluating an existing or planned service, and teaching people about the structures and workings of human services more generally. This makes model coherency a particularly useful approach.
The key issue for model coherency is the needs of service users and the extent to which what a human service does is consistent with addressing those needs. The process of model coherency therefore involves describing and analysing the assumptions upon which the service model is based, the identification of the needs of service users, the content or purpose(s) of the programme, and how the programme actually delivers its services (the programme processes). This might take place in a workshop format as a way of teaching human services or it might be part of a service evaluation or planning process. Model coherency and PASSING together provide a comprehensive process of evaluation and service development.
Model coherency incorporates a ‘theory of needs’ that requires a detailed and exhaustive description and analysis of the needs of clients, taking into account different categories of needs. Universal needs are those needs shared with all human beings, many of which are overlooked when people are redefined as patients or inmates, for example. Fundamental needs are those needs that are relatively more important (e.g. needs for sustenance, safety, belonging, and affiliation) and would usually take priority. Urgent needs are those which, if not met, will make it unlikely that other needs can be addressed (e.g. needs to have high levels of anxiety and insecurity addressed, without which clients would be unable to benefit from other interventions).
Sources of incoherency in human services may come from a mismatch between the assumptions underpinning the service, the identity and needs of the clients, what the service chooses as its purpose, and/or any aspects of the processes adopted by the service. A model coherency analysis is likely to bring such incoherencies to the fore.
CONCLUSION
Normalisation and SRV have contributed much to human service development, particularly for people with learning disabilities where the ideas first emerged. Although more than 3 decades old and following unprecedented reform and changes in services, the ideas remain challenging and provocative. For that reason, and because SRV theory in particular is comprehensive and complex, they are not well understood and often misunderstood. This is a very brief account of both and should be supplemented by the extensive literature available and, if possible, by participation in training workshops. This article has been confined to articulating normalisation and SRV and does not provide a critical analysis, which would be a subject for a further paper.
REFERENCES
- Heller HW, Spooner F, Enright BE, Haney K, Schilit J. Classic articles: a reflection into the field of mental retardation. Educ Training Ment Retard 1991;26:202-206.
- Wolfensberger W. The principle of normalization in human services. Toronto: National Institute on Mental Retardation;1972.
- Wolfensberger W. Social role valorization: a proposed new term for the principle of normalization. Ment Retard 1983;21(6):234-239.
- Kugel RB, Wolfensberger W. Changing patterns in residential services for the mentally retarded. Washington, DC: President’s Committee on Mental Retardation;1969.
- Nirje B. The normalization principle papers. Uppsala, Sweden: Centre for Handicap Research (Uppsala University);1992.
- Goffman E. Asylums: Essays on the social situation of mental patients and other inmates. Harmondsworth: Penguin;1968.
- Race DG. Social role valorization and the English experience. London: Whiting & Birch Ltd;1999.
- Wolfensberger W. A brief introduction to social role valorization: a high-order concept for addressing the plight of societally devalued people, and for structuring human services. 3rd ed. Syracuse, NY: Training Institute for Human Service Planning, Leadership and Change Agentry (Syracuse University);1998.
- Cocks E. An introduction to intellectual disability in Australia. 3rd ed. Canberra, Australia: Australian Institute on Intellectual Disability; 1998.
- Flynn RJ, Lemay RA. A quarter-century of normalization and social role valorization: evolution and impact. Ottawa: University of Ottawa Press;1999.
- Wolfensberger W. A brief overview of social role valorization. Ment Retard 2000;38:105-123.
- Wolfensberger W, Glenn L. Program analysis of service systems (PASS): a method for the quantitative evaluation of human services. Vol. 1 Handbook; Vol. 3 Field Manual. 3rd ed. Toronto: National Institute on Mental Retardation;1975.
- Wolfensberger W, Thomas S. PASSING (program analysis of service systems’ implementation of nor malization goals): normalization criteria and ratings manual. 2nd ed. Toronto: National Institute on Mental Retardation;1983.
- Cocks E. Evaluating the quality of residential services for people with disabilities using program analysis of service systems’ implementation of normalization goals (PASSING). Asia Pac J Disabil 1998;1(2):29-42.
- Flynn RJ, Guirguis M, Wolfensberger W, Cocks E. Cross-validated factor structures and factor-based subscales for PASS and PASSING. Ment Retard 1999;37;281-296.
Dr Errol Cocks, BA MPsych PhD MAPS CPsychol, Professor of Learning Disabilities, Centre for Clinical Psychology and Health Care Research, University of Northumbria, Newcastle, and Consultant Clinical Psychologist and Trust Research and Development Lead, Northgate & Prudhoe NHS Trust, Newcastle, UK.
Address for correspondence: Dr Errol Cocks
Professor of Learning Disabilities
Centre for Clinical Psychology and Health Care Research
University of Northumbria
Newcastle
UK