
East Asian Arch Psychiatry 2016;26:3-9
ORIGINAL ARTICLE
Dr Susmita Halder, PhD, Institute of Behaviour and Allied Sciences, Amity University, Jaipur, India.
Dr Akash Kumar Mahato, PhD, Department of Clinical Psychology, Sweekaar Academy of Rehabilitation Sciences, Secunderabad, Telangana, India.
Address for correspondence: Dr Akash Kumar Mahato, PhD, Department of Clinical Psychology, Sweekaar Academy of Rehabilitation Sciences, Secunderabad TS 500003, India.
Tel: (91) 8003046416; Email: akashmahatocp@gmail.com
Submitted: 17 November 2015; Accepted: 12 April 2016
Abstract
Introduction: Suicide has become an important public health concern with a high number of deaths and increasing number of attempted suicides every year. There are multiple factors that underlie a suicide attempt. Although mental illness and severe stress have long been known to be associated with suicide, socio-demographic and clinical characteristics of those attempting suicide can also provide indications of suicidal intent. The present study aimed to explore the socio-demographic and clinical characteristics of patients in Kolkata, India who attempted suicide.
Methods: Consecutive patients (n = 100) with failed suicide attempt who were referred to the psychiatry department of 2 multispecialty hospitals in Kolkata were included in the study. Their socio-demographic details and clinical characteristics were recorded. Suicidal intent and depressive symptoms were assessed and psychosocial risk factors were identified following detailed clinical interview.
Results: Suicide attempt was more frequent among younger female patients. Reaction to stress was the most common risk factor. The majority of attempts were impulsive in nature rather than planned.
Conclusion: Young adults under stress are more vulnerable. Early identification of such individuals and psychosocial support to prevent suicidal ideation is vital.
Key words: Risk factors; Socioeconomic factors; Suicide, attempted
Introduction
Suicide is the result of an act deliberately initiated and performed by a person in the full knowledge or expectation of its fatal outcome.1 Suicide was the fifteenth leading cause of death in 2012, accounting for 1.4% of all deaths worldwide.2 Suicide is also the cause of almost half of all violent deaths and results in over 0.8 million deaths every year worldwide. It is the second leading cause of death in 15-to-29-year-olds, with indications that for each adult who died of suicide there may have been more than 20 others who attempted suicide.2 A suicidal act that does not end in death is commonly called a suicide attempt or a suicidal gesture.3 Nevertheless, it is equally important as it could indicate distress of the individual, a risk of repetition of the act, and, importantly, a chance for intervention. It is unknown whether socio-demographic and clinical data of suicide attempters have some predictive value. Literature about suicide attempters as well as completed suicides paints an alarming picture. It is suggested that around 25% of suicides are preceded by non-fatal self-harm in the previous year.4 Other studies have put this figure as high as 40%. Although data may vary across studies, they do suggest a significant increase in risk of death due to suicide in repeat attempters.5-11
As per the National Crime Records Bureau, a total of 131,666 people in India committed suicide in 2014. Of these, 14,310 (10.9%) were from West Bengal which was behind Maharashtra (12.4%) and Tamil Nadu (12.2%) in total country-wide suicides.12 Thus, it becomes important to explore the factors that underlie suicide attempts in different geographical areas. There is a growing volume of studies in India on socio-demographic characteristics of suicide attempters and risk factors for suicide but these may vary for different regions. There is a need to obtain data relevant to a particular region, especially in the current environment where suicide is considered a major public health concern.
The present study aimed to explore the various socio-demographic and clinical characteristics of suicide attempters from Kolkata, the capital of West Bengal state, India.
Methods
This was a cross-sectional, hospital-based study conducted in the psychiatry department of Fortis Hospital and Medica Superspecialty Hospital, Kolkata from January 2013 to December 2014. The hospitals cater to clients of Kolkata, and are easily accessible from all parts of the city.
Procedure
Consecutive cases of attempted suicide referred to the psychiatry department from the emergency ward of the hospitals were included in the study. The sample comprised 100 men and women. Patients were reviewed by a consultant psychiatrist and a certified clinical psychologist, and any psychiatric morbidity as per the ICD-10 was diagnosed after taking a clinical history and completion of a mental state examination. Patients were interviewed after obtaining informed consent, and after they were stable and cooperative. The socio-demographic and clinical data sheet was completed. Information was corroborated by informants regarding the circumstances surrounding the suicide attempt. Appropriate pharmacological and psychological interventions were given to the patient.
Socio-demographic Data Sheet
A semi-structured proforma was designed for this study. This sheet contained information about various socio- demographic variables of the sample, including age, gender, religion, education, marital status, domicile, and occupation.
Beck Suicide Intent Scale
The Beck Suicide Intent Scale14 is a 15-item questionnaire designed to assess the severity of suicidal intent in suicide attempters. Each item is scored on a scale of 0 to 2, giving a total score of 0 to 30, with higher scores indicating higher suicidal intent.
Semi-structured Interview
An individual detailed interview was also conducted. The interview focused on details of the suicide attempt in relation to the prevailing situation and circumstances: suicidal intent, number of attempts, history of attempts, and family history.
Results
Suicide attempters were aged 15 to 40 years, with a mean of 23.51 years. The majority of attempters were female (72%) and single (69%). It is worth noting that the majority (42%) were students and graduates (56%). Almost a quarter of the sample had attended postgraduate education. The majority hailed from an urban background (56%). This was primarily because the place of study was Kolkata (Table 1).

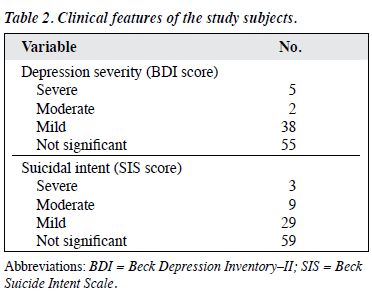
Although 55% of the sample reported no significant depression as per BDI rating, 38% reported a mild level of depression and only 7% a moderate-to-severe level of depression. Suicidal intent was non-significant in 59% of the sample and moderate to severe in 12% (Table 2).

Discussion
Age
Young adults comprised the majority of the study sample. This is consistent with previous findings that suggest a high rate of suicide attempts among adolescents and young adults in eastern India.15 The recent national data also reveal the highest rate of suicide in persons aged 18 to 30 years compared with any other age-group.12 This is contrary to the research findings from western countries that report higher rates of suicide in the elderly. There might have several reasons. The high risk of suicide among the elderly is often attributed to feelings of loneliness and social isolation.16
The feeling of isolation has also been reported as a potential precipitating factor for suicide attempts by the elderly in Asian countries.17 Indian families have a relatively different psychosocial fabric and social isolation is not such a problem because extended family households are still predominant in rural as well as urban areas.18 Researchers have also highlighted the difference among suicide rates in elderly versus young individuals in the West compared with Asian countries. The elderly tend to be more medically fragile and their suicide attempt is often with strong intent and long planned. Thus, they are more likely to achieve a successful (fatal) outcome than their younger counterparts.18
Certain longitudinal studies from India have reported only 47 elderly people over 60 years attempting suicide among 6312 suicide attempters.19 As per official records, 9761 elderly people over 60 years committed suicide all over India, against 44,883 young adults in the age range of 18 to 30 years.12 This suggests that although suicide attempts or suicides are high in the elderly population, the ratio is relatively lower in India.
Gender
It is difficult to pinpoint the relative importance of individual socio-demographic variables in suicide or suicide attempt, but females are known to have a higher rate of suicide attempts than males. The predominance of females in our sample is supported by the fact that males have an approximately 4 times higher rate of successful suicide than women. Nonetheless, women are more likely to attempt suicide than men,20 thus a predominance of female subjects as attempters. The findings of the present study are supported by Bharati et al15 who reported 69% of suicide attempters to be female in their study at a rural hospital in West Bengal. Nonetheless, other studies have reported more suicide attempts in males.21-23 The variation in these findings could be attributed to changing perspectives in society.
Education and Occupation
It is often inferred that higher education indicates a higher level of intelligence, resilience, and competency to deal with difficult situations. Nevertheless, by considering the education level of the studied sample, it is difficult to conclude whether education level was a deterrent in suicide attempt. Studies in places close to Kolkata have reported that 41% of the study sample attempting suicide had been educated up to grade 10 and above.15 More strikingly, the same study revealed that students constituted 47% of 156 suicide attempters. This figure was close to 42% in our total sample. India is a growing economy that is experiencing a rise in many sectors including education. Nonetheless, despite a rise in the national economy, the same cannot be said for employment rates. Researchers have commented on the higher rate of open unemployment in Kolkata and perhaps the waste of human resources is greater here than in any other urban centre in India.24 Lack of adequate jobs and the pressure of competing with an ever increasing number of applicants for jobs takes a significant toll on young adults. Some graduates are devastated when, despite having a well-respected professional degree, they are offered jobs unsuitable to their profile or with too low remuneration. A large number of subjects in our sample reported academic and career issues. This pattern also finds support from data from neighbouring countries such as Nepal that has a similar sociocultural makeup to India, and finds an increased number in suicide attempts among students, particularly after high school and senior secondary examinations. Nonetheless, here the reason appears to be more education- related25 rather than due to familial or relationship problems as in our study sample.
In the present study, housewives constituted 20% of the sample, but they also comprised 27% of the total female subjects who dominated the total sample and most commonly cited relationship issues as the reason for suicide attempt. Working people and those involved in business comprised 24% of the sample. Among these, some cited acute financial problems.
Clinical Characteristics and Reasons
Suicidal intent was not significant in most (59%) cases. This could be because the interview took place when the patient had stabilised after the attempt. Irrespective of this, the subjects remain a vulnerable population of reattempting suicide since the remaining 41% had suicidal intent of varying levels of severity. Reaction to severe stress was the largest single cause, cumulatively accounting for 95% of reasons given by attempters, particularly familial or relationship problems (53%). A substantial number of subjects (38%), mostly students, attempted suicide due to relationship troubles or educational or career difficulties. In a recent study of female college students from Kolkata and surrounding areas, traumatic breakup of a romantic relationship was reported as significantly important in provoking suicidal ideation, second only to sexual assault.26
This corroborates our study findings where relationship trouble was reported by more than half of the total sample. It may be conjecture to comment that a rapid increase in online social networking among young adults has made them more aloof and inept at dealing with exigencies arising out of relationship breakups in the virtual world. Nonetheless, certain studies conclude that social media may pose a risk to vulnerable groups who are part of these virtual communities.27 The findings are also supported by previous studies that imply inter-personal conflict, financial stressors, and educational burden among the most common triggers for attempted suicide.28-31
Mental illness is known to be one of the highest risk factors for suicide.32,33 In the present sample 4% were diagnosed with depressive illness and 1% had psychosis. Although in the present sample 45% of subjects reported a significant level of depression, as rated through BDI scores, only 7% had a moderate-to-severe level of depression. This suggests that the majority of subjects who reported significant depressive features on BDI were depressed at a subsyndromal level and the depression was of transient nature. This was corroborated by the non-significant suicidal intent of 59% of the sample.
None of the individuals in this study identified any of the more commonly cited reasons for their suicide attempt, for example, physical illness. This could be primarily because most were young or adolescent and unlikely to have a major illness. This is further evidenced by data from 2014 that revealed illness as the cause of 18% of suicides across India.12 Despite this, West Bengal had a much lower reporting of illness as the reason for suicide and was not one of the top 10 states to report more than the national average number of suicides.12
Alcohol consumption is another known risk factor for suicide or suicide attempts but none of our study subjects had consumed any alcohol prior to their suicide attempt. This is in contrast with findings of other studies from the state of West Bengal where alcohol had sometimes been consumed by students before the suicide attempt. Nonetheless, these subjects were drawn from a rural rather than urban population.34 Consuming alcohol increases the success of a suicide attempt. Very few cases are reported to hospitals.
Decision and Mode of Attempt
Although impulsivity is one of the variables that enhances the risk of suicide among vulnerable groups,20 there are mixed views regarding the role of impulsivity in suicidal behaviour. Certain studies imply a significant role,35 but others imply a varying degree of impulsive aggressive behaviour in suicide attempts with age playing a confounding role.36 Considering the high ratio of young, mostly female, students (42%) in the sample and reported acute stress due to interpersonal difficulties, impulsiveness regarding a decision to attempt suicide may be understandable and infer a non-serious intent of the suicide attempt.
While overdose with a prescribed drug or consuming poison (71%) was the most frequent means of attempting suicide, hanging and strangulation methods (20%) were reported more than cutting and slashing (9%). The latter were relatively less lethal. This raises questions about the suicidal intent of the attempters and reiterates the impulsivity of some attempts. Nevertheless, the subject’s inability to cope with stress and their inclination to take extreme measures that one day may prove fatal should not be overlooked. This is also important when one considers the high risk of repeat suicidal behaviour during the first year following a suicide attempt, and especially within the first 3 to 6 months.37-39
Limitations
The study has several limitations. The main limitation is that it was a hospital-based cross-sectional study.
Community-based longitudinal studies can reveal more factors and avoid selection bias. It is difficult to make broad generalisations because of the small sample size and data collected were based on verbal responses of the sample subjects. It comprised subjects from largely urban and semi- urban areas, very few from rural areas, and thus may not be representative of the population. Suicide attempt in India is an act punishable by law although the government has been trying to repeal it. It also carries a stigma. Many attempts go unreported. This study reports only those cases reported to the hospitals and there was no control group. Considering the limited hospital stay of the subjects, detailed personality assessment of the subjects was not possible but might have provided vital therapeutic inputs. Although the subjects were given therapeutic counselling after their mood stabilised, they were not followed up for long.
Conclusion
Young females formed the majority of suicide attempters. Most reported depression at a subsyndromal level. This explains why only a small percentage of the attempts was planned and most were carried out on impulse without a firm intention of committing suicide. Reaction to severe stress, mostly due to inter-personal reasons, was the most common triggering factor. Inferring a non-serious intent in the attempters, suicide attempts can be taken as a cry for help and also demonstrate and individual’s poor coping skills and ability to handle extreme situations. Irrespective of the causes, the findings suggest that adolescents and young adults, mostly females, were at highest risk. These findings highlight the vital role played by parents and teachers in supporting their pupils and children in stressful situations. The findings reiterate the role of early identification, prevention, and psychosocial intervention in patients with suicide attempts. Successful suicide cannot be treated.
Declaration
The authors declared no conflict of interest in this study.
References
- World Health Organization. The World Health Report 2001. Available from: http://www.who.int/whr/2001/chapter2/en/index6. html. Accessed 20 Sep 2015.
- World Health Organization. Preventing suicide: A global imperative. 2014. Available from: http://www.who.int/mental_health/suicide- prevention/world_report_2014/en/. Accessed 20 Sep 2015.
- Michello C, Lynne FG, Lemyra D. Suicidality: nomenclature. In: Claire MR, Jeffrey LE, editors. Encyclopedia of interpersonal violence. Sage Publications; 2008: 701-2.
- Owens D, House A. General hospital services for deliberate self-harm. Haphazard clinical provision, little research, no central strategy. J R Coll Physicians Lond 1994;28:370-1.
- Kerkhof AJ, Arensman E. Attempted suicide and deliberate self-harm: epidemiology and risk factors. In: Gelder MG, López-Ibor JJ, Nancy A, editors. New Oxford textbook of psychiatry, E-book. 4.15.2. Oxford University Press; 2000.
- De Moore GM, Robertson AR. Suicide in the 18 years after deliberate self-harm: a prospective study. Br J Psychiatry 1996;169:489-94.
- Jenkins GR, Hale R, Papanastassiou M, Crawford MJ, Tyrer P. Suicide rate 22 years after parasuicide: cohort study. BMJ 2002;325:1155.
- Owens D, Horrocks J, House A. Fatal and non-fatal repetition of self- harm. Systematic review. Br J Psychiatry 2002;181:193-9.
- Suokas J, Suominen K, Isometsä E, Ostamo A, Lönnqvist J. Long-term risk factors for suicide mortality after attempted suicide — findings of a 14-year follow-up study. Acta Psychiatr Scand 2001;104:117-21.
- Suominen K, Isometsä E, Suokas J, Haukka J, Achte K, Lönnqvist J. Completed suicide after a suicide attempt: a 37-year follow-up study. Am J Psychiatry 2004;161:562-3.
- Tejedor MC, Diaz A, Castillón JJ, Pericay JM. Attempted suicide: repetition and survival — findings of a follow-up study. Acta Psychiatr Scand 1999;100:205-11.
- National Crime Records Bureau. Ministry of Home Affairs, India. Accidental deaths and Suicides in India. 2014. Available from: http://ncrb.gov.in/StatPublications/ADSI/ADSI2014/ADSI2014.asp. Accessed 28 Aug 2015.
- Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory–II. San Antonio, TX: Psychological Corporation; 1996.
- Beck AT, Schuyler D, Herman I. Development of suicidal intent scales. In: Beck AT, Resnik HL, Lettieri DJ, editors. The prediction of suicide. Bowie, MD: Charles Press; 1974: 45-56.
- Bharati S, Mallik S, Datta PP, Mukhopadhyay A, Datta D, Haq S. Socio-demographic profile and suicidal intent of attempted suicide cases: a hospital based study in West Bengal, India. Natl J Med Res 2013;3:122-5.
- Barraclough BM. Suicide in the elderly: recent developments in psychogeriatrics. Br J Psychiatry 1971;Spec Suppl 6:87-97.
- Wong MM, Tsui CF, Li SW, Chan CF, Lau YM. Patients committing suicide whilst under the care of the elderly suicide prevention programme of a regional hospital in Hong Kong. East Asian Arch Psychiatry 2011;21:17-21.
- Garg R, Trivedi JK, Dhyani M. Suicidal behaviour in special population: elderly, women and adolescent in special reference to India. Delhi Psychiatry J 2007;10:106-18.
- Rao AV, Madhavan T. Depression and suicide behaviour in the aged. Indian J Psychiatry 1983;25:251-9.
- Sadock BJ, Sadock VA. Suicide. In: Sadock BJ, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences / clinical psychiatry. 10th ed. Lippincott Williams & Wilkins; 2007: 898-907.
- Ramdurg S, Goyal S, Goyal P, Sagar R, Sharan P. Sociodemographic profile, clinical factors, and mode of attempt in suicide attempters in consultation liaison psychiatry in tertiary care center. Ind Psychiatry J 2011;20:11-6.
- Kumar PN. Age and gender related analysis of psychosocial factors in attempted suicide. Indian J Psychiatry 1998;40:338-45.
- Das PP, Grover S, Avasthi A, Chakrabarthi S, Malhotra S, Kumar S. Intentional self-harm seen in psychiatric referrals in a tertiary care hospital. Indian J Psychiatry 2008;50:187-91.
- Kundu N. The case of Kolkata. Understanding slums: case studies for the global report on human settlements 2003. Available from: http://www.ucl.ac.uk/dpu-projects/Global_Report/pdfs/Kolkata.pdf. Accessed 10 Mar 2016.
- Halder S, Chakravorty PK, Thapa P. Risk factors of suicidal attempts among Napalese adolescents and young adults. A hospital based study. Proceedings of the 4th National Conference of Psychiatrists Association of Nepal; 2010 March 24-25; Kathmandu, Nepal.
- Chatterjee I, Basu J. Perceived causes of suicide, reasons for living and suicidal ideation among students. J Indian Acad Appl Psychol 2010;36:311-6.
- Luxton DD, June JD, Fairall JM. Social media and suicide: a public health perspective. Am J Public Health 2012;102 Suppl 2:S195-200.
- Khan FA, Anand B, Devi MG, Murthy KK. Psychological autopsy of suicide — a cross sectional study. Indian J Psychiatry 2005;47:73-8.
- Sharma RC. Attempted suicide in Himachal Pradesh. Indian J Psychiatry 1998;40:50-4.
- Srivastava MK, Sahoo RN, Ghotekar LH, Dutta S, Danabalan M, Dutta TK, et al. Risk factors associated with attempted suicide: a case control study. Indian J Psychiatry 2004;46:33-8.
- Mohanty S, Sahu G, Mohanty MK, Patnaik M. Suicide in India: a four year retrospective study. J Forensic Leg Med 2007;14:185-9.
- Cavanagh JT, Carson AJ, Sharpe M, Lawrie SM. Psychological autopsy studies of suicide: a systematic review. Psychol Med 2003;33:395-405.
- Balhara YP, Verma R. Schizophrenia and suicide. East Asian Arch Psychiatry 2012;22:126-33.
- Bhattacharjee S, Bhattacharya A, Thakurta RG, Ray P, Singh OP, Sen S. Putative effect of alcohol on suicide attempters: an evaluative study in a tertiary medical college. Indian J Psychol Med 2012;34:371-5.
- Gvion Y, Levi-Belz Y, Hadlaczky G, Apter A. On the role of impulsivity and decision-making in suicidal behavior. World J Psychiatry 2015;5:255-9.
- Turecki G. Dissecting the suicide phenotype: the role of impulsive- aggressive behaviours. J Psychiatry Neurosci 2005;30:398-408.
- Hawton K, Fagg J. Repetition of attempted suicide: the performance of the Edinburgh predictive scales in patients in Oxford. Arch Suicide Res 1995;1:261-72.
- Hawton K, Fagg J. Suicide and other causes of death, following attempted suicide. Br J Psychiatry 1988;152:359-66.
- Goldacre M, Hawton K. Repetition of self-poisoning and subsequent death in adolescents who take overdoses. Br J Psychiatry 1985;146:395-8.
